ST3 Training Map
Your Final GP Post
Twelve months. One chance to become the GP you've always wanted to be. No pressure.
(Okay — some pressure. But you've absolutely got this.)
📥 Downloads
Handouts, tutorial suggestions, and teaching extras — ready when you need them. Use these in tutorials, for self-directed learning, or to rescue a quiet Sunday evening before Monday morning clinic.
path: TUTORIAL SUGGESTIONS FOR ANY STAGE OF GP
- 10 golden rules for general practice.docx
- being therapeutic - laughter as medical therapy.ppt
- being therapeutic - when listening is the therapy - the patients lament - hidden key to effective listening.pdf
- being therapeutic - when listening is the therapy - the patients lament - turning moaning into therapy.pdf
- clinical - clinical examination - is it really necessary (TEACHING RESOURCE).ppt
- clinical - emergencies assessment questionnaire EmAQ.doc
- clinical - spotting the sick child in 3 minutes.doc
- clinical examination as a therapeutic examination.docx
- decisions - cognitive biases.ppt
- decisions - complexity and how doctors think.pdf
- decisions - fast and slow thinking systems.docx
- decisions - how doctors solve problems.docx
- decisions - pattern recognition in the consultation.doc
- decisions - perceptual capacity and the gp.docx
- decisions - prioritising making decisions and managing your time.docx
- decisions - RAPRIOP management options.docx
- decisions - when no diagnostic label is applied.docx
- information technology - using the computer in the consultation.docx
- learning and develoment - core values - what makes you tick.docx
- learning and development - 2 minutes on Educational Change.docx
- learning and development - 2 minutes on Motivation for Learning.docx
- learning and development - feedback - basic principles of.docx
- learning and development - feedback - receiving.docx
- learning and development - keeping clinically up to date - good and bad doctors.doc
- learning and development - learn every day in every way.pdf
- learning and development - motivating values.docx
- learning and development - novels about general practice.docx
- learning and development - personal values - what makes you tick.docx
- learning and development - self actualisation level.docx
- learning and development - self fulfillment - self actualisation index.docx
- learning and development - wheel of life - hows your life currently going.docx
- learning and development - winners and losers - what are you.doc
- mrcgp professional capabilities.docx
- person centred medicine - 5 things all patients want to HAPPEN.ppt
- person centred medicine - 5 things all patients want to KNOW.ppt
- person centred medicine - 5 things all patients want.docx
- person centred medicine - a story (after Candide) - individual vs population medicine.docx
- person centred medicine - being therapeutic by encouraging the narrative thread.docx
- person centred medicine - disease vs illness.docx
- person centred medicine - disease vs illness.ppt
- person centred medicine - how to do it.docx
- person centred medicine - the health belief model.docx
- person centred medicine - triangular thinking in general practice.docx
- person centred medicine - why patients go to the doctor.docx
- politics - how tainted is medicine - the big pharma.doc
- politics - left vs right wing - what does it all mean.doc
- politics - the NHS race.pps
- prescribing - 10 tips for safer prescribing.pdf
- prescribing - high risk medications for causing errors.pdf
- probophilia - quality versus quantity - are we counting the wrong things.pdf
- what makes a good gp - braunack.pdf
- what makes a good gp - leck and leck.pdf
- what makes a good gp - perceptual capacity.doc
- whats a good doctor and how do you make one by rizo et al.docx
- when no diagnostic label is applied by jones et al.docx
Web Resources
A hand-picked mix of official guidance and real-world GP training resources. Because sometimes the best pearls are not hiding in the official documents — though they are hiding pretty effectively.
The ST3 GP Post Training Map — assessments, milestones, and what to achieve across your final 12 months
Quick Summary — If You Only Read One Thing
(including CbDs)
(≥1 Audio-COT)
(3 CCR + 1 other)
AKT + SCA
everything below
all must reach "competent"
The ST3 Essentials at a Glance
- 4 pillars underpin everything: Relationships · Decision-Making · Management · Professionalism
- Exams: Pass AKT and SCA — ideally around the 6-month mark; discuss timing with your trainer/TPD
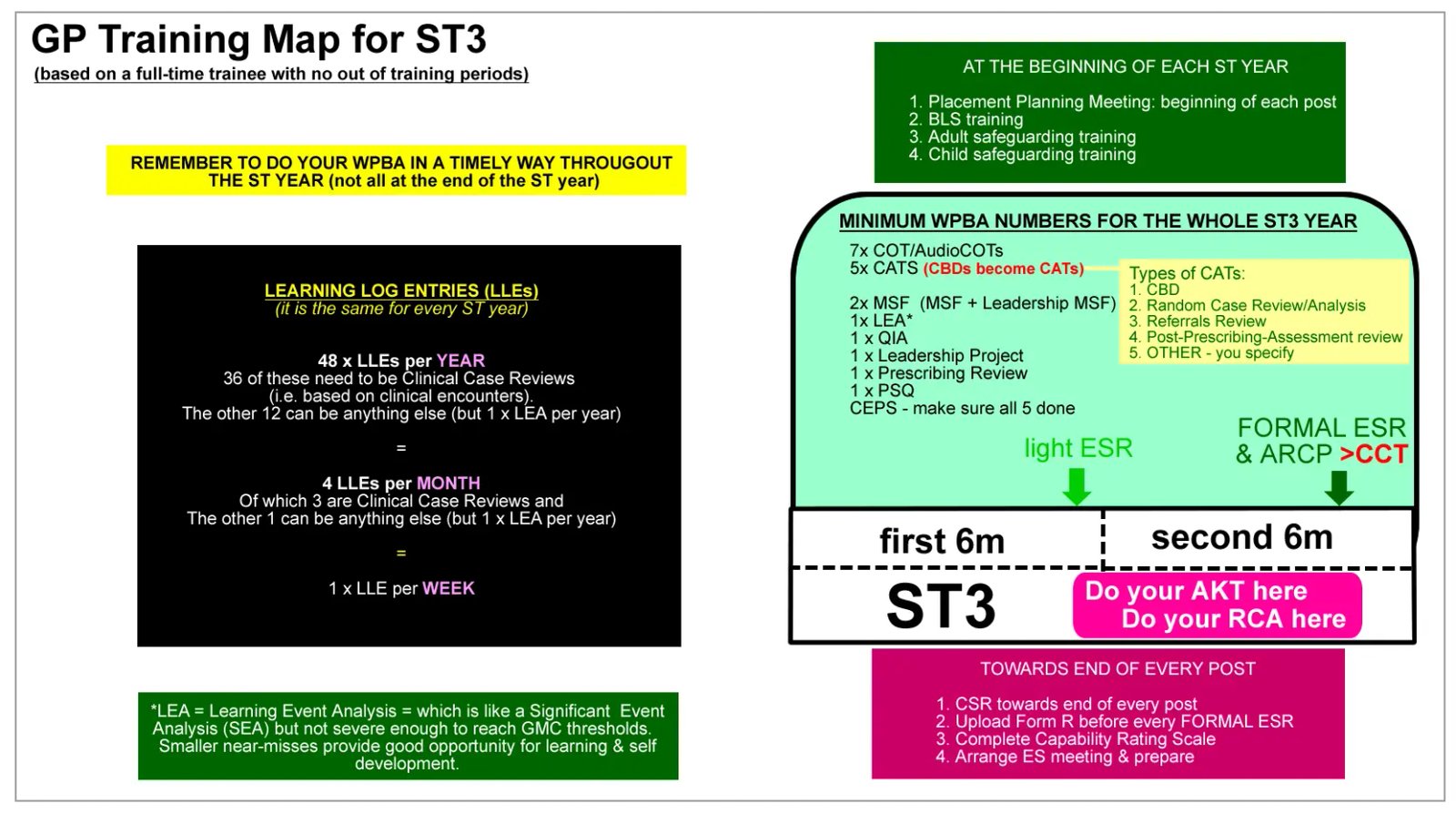
- WPBA numbers: 5 CATs + 7 COTs (≥1 Audio-COT) — spread throughout, never all at the end
- ePortfolio: 4 log entries per month (3 Clinical Case Reviews + 1 other); 1 Learning Event Analysis per year
- Mandatory items: Leadership Project · Prescribing Review · 1 Leadership MSF · 1 PSQ · All CEPs · Compliance Passport
- Performers' List: Apply via PCSE Online no earlier than 6 months before CCT, no later than 3 months before
- UUC / OOH: Check with your Training Programme Administrator — do NOT leave it all to the final weeks
- Final ARCP: All 13 Professional Capabilities must be marked "Competent for Licensing" by your Educational Supervisor
- Compliance Passport: Annual BLS, Defibrillator, Adult Safeguarding, Child Safeguarding — all evidenced in ePortfolio
- IMG note: If English is not your first language — start working on it from day one. The SCA is heavily language-dependent
Why ST3 Really Matters
ST3 is not just "the last year of training." It is the year everything starts coming together: consulting, clinical judgement, risk management, admin systems, urgent care, portfolio evidence, and your identity as a doctor. By the end, you will be making hundreds of clinical decisions daily without a safety net.
You are not expected to know everything. But you are expected to function at the level of a newly qualified independent GP. This is the year when your consultation style either settles into something excellent or calcifies into something mediocre. Use it deliberately.
By the end of ST3, you should be able to:
- Assess most presentations safely without needing constant rescue
- Recognise when something is urgent, serious, or outside your competence
- Manage common primary care problems confidently
- Consult in a patient-centred but efficient way
- Explain diagnoses and plans clearly in plain English
- Work safely with results, letters, prescriptions, and follow-up systems
- Contribute well to the team
- Show good professional judgement in complex situations
- Keep your portfolio, ESR, and ARCP evidence in good order
The ARCP panel does not just look for a pile of forms. It looks for a convincing overall picture that you are ready for licensing.
📈 What "Good ST3 Progress" Looks Like in Real Life
A good ST3 trainee is usually showing the following by the middle and later parts of the post. These are the patterns supervisors and ARCP panels are looking for — not just a completed checklist.
- Needing less frequent interruption help during surgeries
- Becoming more efficient without becoming brusque — safe efficiency, not just speed
- Presenting fewer "what do I do?" cases and more "this is my plan — do you agree?" cases
- Managing admin and clinical workflow more reliably
- Showing more mature uncertainty management — acknowledging unknowns without becoming paralysed by them
- Producing learning logs that demonstrate judgement, not just storytelling
- Doing portfolio evidence steadily instead of reactively
- Being known by the team as dependable, respectful, and safe
The Four Pillars Framework
Every activity in GP training — whether in hospital or in general practice — maps onto three core skill areas, all underpinned by professionalism. Understanding these pillars helps you use your Final Placement Planning Meeting productively, write better learning log entries, and see how your WPBAs fit together.
Relationships
How you communicate with patients and colleagues. Face-to-face and telephone consultations. MDT interactions. This includes ICE, empathy, signposting, shared decision-making, and rapport.
Decision-Making
How you make clinical judgements. Diagnosis, differential diagnoses, investigations, management plans. Managing uncertainty. Knowing when to refer. Recognising your own limits.
Management
How you manage your workload, your time, and yourself. Admin, results, letters, prescriptions. Wellbeing and resilience. Happy, well-grounded doctors make fewer mistakes.
Professionalism
The foundation under all three pillars. Genuine respect for patients, colleagues, and learning. Engagement with ePortfolio and WPBAs not as chores, but as evidence of who you are becoming.
🤝 Relationships — what "competent" looks like by the end of ST3
By the end of ST3, you should be able to:
- Conduct face-to-face consultations of approximately 15 minutes safely and consistently, managing the wider surgery workload — this is the realistic contemporary ST3 target. Early in the year, longer appointments may still be needed while working safely; the goal is safe efficiency, not speed at any cost.
- Run safe and effective telephone consultations — at least one Audio-COT assessed
- Demonstrate ICE exploration routinely — not as a scripted add-on, but as a natural part of every consultation
- Contribute meaningfully in practice meetings rather than just sitting silently at the back
- Receive MSF comments reflecting good working relationships with clinical and non-clinical staff
- Show evidence in ePortfolio log entries of reflecting on specific communication micro-skills: ICE, PSO, signposting, screening, summarising, explanations
🧠 Decision-Making — what "competent" looks like by the end of ST3
- Manage most consultations independently — only occasionally needing to check (like a qualified GP would)
- Make sound working diagnoses most of the time; thinks clearly about differential diagnoses
- Know your "information flow" system — where do you look when you don't know something? (Not always "ask the senior")
- Handle test results and letters safely; do home visits independently
- Show in debriefs that the trainer/supervisor is growing in confidence in your abilities — to the point that not every consultation needs debriefing
- Complete a Prescribing Review Assessment with no significant concerns
⚙️ Management — what "competent" looks like by the end of ST3
- Understand how general practice systems work: clinical, administrative, IT
- Have a personal daily routine for handling tasks, letters, results, and prescriptions — discuss your system with your trainer
- Use the clinical computer system fluently (EMIS, SystmOne, or Vision)
- Prepare adequately for all learning activities — tutorials, HDR, presentations
- Engage in Quality Improvement and complete a mandatory Leadership Project
- Demonstrate good sick leave pattern — not too much and not too little (both can flag self-management issues)
⭐ Professionalism — what "competent" looks like by the end of ST3
- Demonstrate genuine respect for patients — not just in formal assessments, but in everyday interactions
- Respond constructively to negative feedback — this is one of the most important professional skills you can demonstrate
- Write adequate medical records — not one-liners. Consult entries added in a timely way. Never alter records retrospectively. (All systems have an audit trail — they can see every change you make.)
- Treat WPBAs with respect — prepare CBD sheets carefully; give your trainer time and thought-out case selection for COTs
- Show evidence of rationing care: not over-referring, not over-investigating, not treating every ill with a pill
The ST3 Phased Roadmap
Think of ST3 as five overlapping phases rather than twelve separate months. Each phase builds on the last. The roadmap below gives you a clear sense of what to focus on and when.
Settle in & orient
Build & plan
Deepen & assess
Consolidate & complete
Final stretch & sign-off
Understand the Professional Capabilities (13 PCs)
The Professional Capabilities (previously called "competences") are the 13 areas you are measured against throughout GP training. Nearly everything you do maps onto these 13 PCs.
By ST3, you should have a solid understanding of them. If you'd like a quick recap, the Bradford VTS cheat sheet is the fastest way to orientate yourself.
Professional Capabilities Cheat Sheet →Revisit learning log entry principles
ARCP panels and Educational Supervisors primarily assess you through your ePortfolio — and log entries are the core of it. Log entries must show evidence of performance and of learning. Write them as though someone who doesn't know you will be reading them, because at ARCP time, that is exactly what happens.
Use the ISCE framework to structure entries:
- I — Information about the situation (enough context to understand it)
- S — Self-awareness (how did it make you feel? what were your thoughts?)
- C — Critical analysis (making sense of it; what does it mean?)
- E — Evidence of learning (what will you do differently? what has changed?)
Sit in with different staff (if you haven't already)
If you didn't get this opportunity in your previous GP post, now is the time. Ask your trainer to arrange short sessions (1–1.5 hours each) with:
- Practice nurses and nurse practitioners
- Clinical pharmacist
- District nurses and health visitors
- Practice manager and admin staff
- Midwife (antenatal clinics)
Use the Bradford VTS task sheets (in the GP Post Induction downloads) to make the most of these sessions rather than just sitting and watching.
GP Post Induction Page →Establish your daily work routine
Without a routine, things get missed. Clinical mistakes and errors follow. Discuss with your trainer what their own post-surgery routine looks like. Then build yours. A typical routine after a surgery might look like:
- Clinical tasks (action items from the session)
- Scanned clinical letters — read and file
- Blood and investigation results
- Physical pigeon hole
- Work email
Your system will evolve. That's fine. The key thing is having one.
Get comfortable with the clinical computer system
Most practices use EMIS, SystmOne, or Vision. Ask your Practice Manager for the "test patient" — every system has one. Explore it without the pressure of a real clinical encounter. Watch YouTube tutorials for your specific system.
Ask about add-on systems like ARDENS and ASSIST, which many practices use. Get someone to show you how they work.
If you type slowly — learn properly, now. You will not survive general practice without reasonable typing speed. Try TypingClub.com or Mavis Beacon. Yes, really.
Log into FourteenFish and orientate yourself
Log in 3–4 times in the first two weeks just to get a feel for the layout. Once the system is familiar, adding log entries becomes much easier. It's horrible trying to write up a meaningful learning experience when you're simultaneously confused about which button to press.
FourteenFish ePortfolio →Start your English language plan (if needed)
This applies primarily to doctors who qualified outside the UK. Ask yourself honestly: "Do I need to improve my spoken English?" If yes — start now. The SCA is heavily dependent on natural, fluent English communication. The examiners are patients; if they can't understand you or if your responses sound stilted, you will lose marks regardless of clinical knowledge.
A combined approach works best:
- Watch English TV series (without subtitles)
- Listen to audiobooks in English
- Speak English as much as possible outside of work, not just during it
- Consider a language class or conversation partner
- Read medical story books aloud — This is Going to Hurt by Adam Kay is a good start
Plan your courses in advance
Practices cannot release you at the last minute for courses. Book with at least 6 weeks' notice. Courses to consider at this stage:
- BLS and adult/child safeguarding courses (mandatory — get them early)
- GP knowledge update course (NB Medical, Red Whale, etc.)
- AKT preparation course
- SCA preparation course
- Consultation skills training
- Specific knowledge areas: contraception, ECGs, spirometry, diabetes, COPD
- Urgent and Unscheduled Care course (Out of Hours preparation)
- IMG-specific courses if applicable
Start (or continue) reading a consultation book
A good consultation book will transform your clinical practice far more than another revision resource. These are particularly recommended for ST3:
| Book | Best for |
|---|---|
| Bedside Matters — Peter Tate & Francesca Frame (2020) | Novel-style, excellent reviews, covers real GP situations |
| The Naked Consultation — Liz Moulton | Straight to the point; covers difficult situations well |
| Skills for Communicating with Patients — Silverman et al | Evidence-based; best reserved for ST3 (heavy for ST1/2) |
| Consulting in a Nutshell — Roger Neighbour (2020) | 3-step approach; sections on difficult consultations |
| The Modern Guide to GP Consulting — Alex Watson | Short, straight-to-point, Six S for Success framework |
Start your ePortfolio: aim for 4 log entries per month
The target is 4 log entries per month:
- 3 on a clinical encounter with a patient (recorded as Clinical Case Reviews)
- 1 on anything else — an HDR session, a difficult situation, a reflection on a team meeting
Make the last week of every month your "non-clinical log entry" week — it creates a simple rhythm. Get your trainer to look at your early entries and give honest feedback on reflection quality. Better to fix your approach in month 2 than in month 10.
Begin CATs and COTs — start early, spread them out
By the end of ST3 you need: 5 CATs and 7 COTs (at least 1 Audio-COT).
The most common mistake trainees make is leaving these until the final 2 months. This causes stress, rushed assessments, and poor-quality feedback. Start in month 2. Aim for roughly one CAT or COT every 4–6 weeks.
CBD/CAT Resources → COT Resources →Learn how to study effectively — seriously
Most doctors were never taught how to study well. Research shows that many of our "default" study methods (e.g. re-reading, highlighting) are among the least effective. The most effective methods — spaced repetition, active recall, interleaving — are rarely taught at medical school.
Read the Bradford VTS page on effective studying and discuss with your trainer. Then implement it. This matters especially for AKT preparation.
How to Study Effectively →Register for AKT and SCA
Don't leave registration late — exam dates fill up. Discuss timing with your trainer and TPD. A common approach is to sit both AKT and SCA around the 6-month mark, since the clinical knowledge needed for AKT also underpins SCA performance.
- Join an AKT trainee study group — being in a group is significantly correlated with passing
- Join an SCA practice group — regular case practice with peers is the single most valuable SCA preparation activity
- Consider an AKT prep course and/or online revision platform
Think about your PDPs
Every GP trainee writes PDPs (Personal Development Plans) for each post. Usually 3–5 items. They must be SMART:
| Letter | Meaning | Example |
|---|---|---|
| S | Specific | "Improve my knowledge of contraception" not "improve clinical knowledge" |
| M | Measurable | "Attend a contraception course" |
| A | Attainable | Attending a course is doable. Reading 10 books is not. |
| R | Realistic | "Read a consultation book over 3 months" not "by next week" |
| T | Time-bound | Set a specific deadline, not "eventually" |
You will continue writing PDPs every year as a qualified GP for your annual appraisal. Think of ST3 PDPs as practice for a lifetime habit.
Good ST3 PDP themes — these are relevant, achievable, and linked to real GP needs:
- Improving dermatology diagnosis and management in primary care
- Safer prescribing in older adults and polypharmacy situations
- Improving telephone and remote consulting skills
- Managing same-day urgent presentations more confidently
- Improving women's health, contraception, and HRT skills
- Improving musculoskeletal assessment in primary care
- Consulting more efficiently at 15-minute appointments
- Improving admin workflow and result handling systems
Intensify AKT and SCA preparation
By month 3, you should have a clear revision plan in place for both exams. Many trainees find it helpful to take both AKT and SCA in the same sitting window — the clinical knowledge they overlap significantly.
- Do regular mock AKT questions — aim for a block of 20–30 questions every 2–3 days minimum
- Practise SCA cases with peers at least once a week — ideally with feedback from a trainer or senior colleague
- Go on a GP knowledge update course (NB Medical, Red Whale) to refresh clinical knowledge breadth
- Join an online SCA prep platform
Start your Leadership Project
The Leadership Project is MANDATORY. Non-negotiable. It is best started now — in months 3–6 — so that it is well underway before the exam pressure peaks in the second half of ST3.
Tips for choosing a project:
- Keep it simple — small, well-executed projects score better than ambitious, incomplete ones
- Pick something you find genuinely interesting — you'll do it better
- Discuss options with your trainer. They have seen what works and what doesn't
- It can be a QI project, a clinical audit, an educational initiative, or a service improvement
Concrete examples that work well:
- Improving a recall system for a chronic disease (e.g. missed annual reviews)
- Improving a repeat prescribing safety step
- Improving a results workflow or documentation process
- Improving trainee induction information
- Improving coding or documentation in one clinical area
- Improving how practice teaching sessions are organised
Continue WPBAs — aim for a steady pace
By month 6, you should have at least 2–3 CATs and 3–4 COTs completed. The responsibility for arranging these rests entirely with you — your trainer will not chase you. Your trainer is deliberately stepping back to encourage autonomous learning.
Consider teaching a session at HDR
Effective teaching is a skill — not something you just get up and do. If you are asked (or want) to present at HDR or a practice meeting, take time to learn some basic teaching theory first. You will deliver a much better session, and you'll understand why certain approaches work better than others.
Teaching for Beginners →Engage with UUC / Out of Hours
UUC (Urgent Unscheduled Care) experience is gained through being the on-call duty doctor during normal hours AND/OR through Out of Hours (OOH) sessions.
Good practice guidance:
- Do NOT leave all your OOH sessions to the final months of ST3 — it's stressful, and it shows poor time management on the ePortfolio
- Tell the practice before any OOH session so they can arrange time off — you must not exceed 40 hours per week
- Write up each OOH session in the ePortfolio, reflecting on at least one or more UUC capability
- Check with your Training Programme Administrator how many sessions your deanery requires
ESR mid-point — Educational Supervision Review
Your ES meetings feed directly into ARCP panels. Prepare thoroughly. Allow 2–3 hours for the meeting. The three key areas of the ES prep form are:
- "Finding the evidence for the Capability Self-Rating Scales" — think carefully and specifically about what your ePortfolio entries show for each of the 13 PCs
- "Formulating action points for the capabilities" — what do you still need to work on?
- PDPs — review progress on existing ones and update for the next period
Also ask your Clinical Supervisor to complete a CSR (Clinical Supervisor's Review).
Educational Supervision Guide →Attempt AKT and SCA exams
Around the 6-month mark is a commonly recommended time to attempt both AKT and SCA. You have enough clinical experience to feel confident, but enough time remaining in training to resit if needed.
If you don't pass first time — pick yourself up, analyse what went wrong specifically, and make a clear improvement plan with your trainer. Many excellent GPs did not pass first time. What matters is how you respond.
AKT Resources → SCA Resources →Complete your Prescribing Review
The Prescribing Review is MANDATORY. It exists because patient harm from poor prescribing is a significant and preventable problem in primary care. Use it as a genuine opportunity to review your habits — not just as a form to complete.
Specific areas worth reviewing in the prescribing assessment:
- Antibiotic choice and duration — are you following local formulary and NICE guidance?
- High-risk prescribing — NSAIDs in renal impairment, anticoagulants, lithium, methotrexate
- Polypharmacy in older adults — are all medications still indicated and monitored?
- Renal function awareness — are you adjusting doses appropriately?
- Contraception and HRT prescribing confidence — common gaps for trainees
- Monitoring requirements — are review intervals in place for long-term medications?
- Safer documentation and review intervals in repeat prescribing
Do your MSF and PSQ
In the final ST3 year you need:
- 1 regular MSF — aim to complete this in the first 6 months of ST3. Needs at least 10 respondents, normally including both clinicians and non-clinicians. Sending to only doctors and missing admin/nursing staff is a common gap.
- 1 Leadership MSF — complete this in the second 6 months, after your leadership activity. Specifically gathers feedback on your leadership behaviours during the project.
- 1 PSQ (Patient Satisfaction Questionnaire) — choose your timing sensibly. Do not send PSQs when your admin systems are chaotic, you are running very late, or the team has not properly organised distribution. The quality of your PSQ data depends heavily on how it is administered.
Continue and complete remaining WPBAs
By month 9, you should have completed or nearly completed your 5 CATs and 7 COTs. Use this phase to fill any gaps. Remember: at least one COT must be an Audio-COT. If you haven't done one yet — now is the time.
Audio-COT Guide →Apply to the Performers' List — between 6 and 3 months before CCT
This is the window in which to apply: no earlier than 6 months before CCT, no later than 3 months before. If you miss this window, you may not be able to work independently when you qualify. See the dedicated Performers' List section of this page for full details.
Is your ePortfolio ARCP-ready?
In the final stretch, stop thinking only in terms of "what have I done?" and start thinking "would an ARCP panel clearly see I am ready for independent practice?"
Ask yourself:
- Are my assessments spread sensibly across the year — or all bunched at the end?
- Do I have enough convincing evidence across all capabilities — not just the obvious clinical ones?
- Do my logs show progression and learning, not just repetition of similar entries?
- Is my ESR likely to support "Competent for Licensing" across all 13 PCs?
- Have I completed leadership activity, Leadership MSF, PSQ, Prescribing Review, and QIA?
- Is my CEPS evidence broad enough — including observed intimate examinations?
- Is my UUC evidence convincing — genuine range, real reflection?
- Have I passed (or appropriately planned for) AKT and SCA?
- Is my Compliance Passport complete — including Form R?
4 log entries per month (3 CCR + 1 other) — maintained throughout; at least 1 Learning Event Analysis this ST year.
Complete ALL WPBAs — final checks
Final checklist:
- 5 CATs ✓
- 7 COTs (at least 1 Audio-COT) ✓
- 1 Leadership MSF ✓
- 1 PSQ ✓
- Prescribing Review ✓
- Leadership Project ✓
- All CEPs completed and evidenced ✓
If anything is missing — this is your last chance. Get it done immediately.
CEPs Page →Compliance Passport — annual mandatory training
In the last 12 months you must have evidence of completing the following (with a log entry for each):
- BLS training
- Defibrillator / AED training
- Adult Safeguarding update
- Child Safeguarding update
Also strongly recommended (and mandatory for ongoing GP practice): PREVENT training. Often covered within Adult Safeguarding courses.
Other "boring but essential" compliance items often missed:
- Form R / required declarations — ensure your Form R is current and accurate
- Time out of training accuracy — any periods of leave or absence must be correctly recorded; inaccuracies cause ARCP complications
- Evidence attached in the right place on your ePortfolio — certificates filed in the wrong section don't count
- CEPS evidence — broad enough, including observed intimate examinations by end of ST3
Have you passed AKT and SCA?
If yes — brilliant. If not:
- This is your final window for a resit before your planned CCT date
- Analyse your performance feedback honestly — what specifically went wrong?
- Do more mock SCA cases / AKT question banks
- If you cannot pass in time, discuss with your TPD about a training extension
Final ESR and CSR — your most important ES meeting
Treat this as your most important ES meeting. The outcome feeds directly into your ARCP sign-off panel. Prepare exceptionally carefully.
Two critical areas to focus on:
- Capability Self-Rating Scales: For CCT sign-off, all 13 PCs must be rated "Competent for Licensing" by your Educational Supervisor. Know which ones are borderline and address them specifically in the meeting.
- PDPs for your first year as a qualified GP: Write PDPs that are relevant to the scope of work you will be doing post-CCT. These can be transferred directly into your first GP appraisal portfolio.
Ask your Clinical Supervisor to complete a CSR before the meeting.
Mandatory Requirements — Complete Checklist
Every item below is non-negotiable. If any are missing at your final ARCP, you cannot be signed off for CCT. Print this. Stick it on your fridge. Look at it monthly.
| Requirement | Minimum | Key Notes | When to Complete |
|---|---|---|---|
| CATs (Care Assessment Tools) | 5 | Includes CbDs and other CAT types (Random Case Review, Referrals Review, etc.) | Spread throughout ST3 — start month 2 |
| COTs (Consultation Observation Tools) | 7 | At least 1 must be an Audio-COT | Spread throughout ST3 — start month 2 |
| Log Entries | 4/mo | 3 CCRs + 1 other per month. 1 Learning Event Analysis per year | Ongoing — every week |
| Leadership MSF | 1 | Multi-Source Feedback specifically on leadership skills (from project) | After completing Leadership Project |
| PSQ (Patient Satisfaction Questionnaire) | 1 | From real patients in clinical practice | Months 6–10 |
| Leadership Project | 1 | QI, audit, service improvement, or educational initiative | Start months 3–6; complete by month 9 |
| Prescribing Review | 1 | Assessment of prescribing safety and habits — no significant concerns | Months 4–9 |
| CEPs (Clinical Examination & Procedural Skills) | All required | All mandatory CEPs must be completed and evidenced in ePortfolio | Throughout training — complete by month 10 |
| UUC / Out of Hours sessions | As per contract | Check with Training Programme Administrator — contractual sessions are mandatory | Spread throughout — NOT all at the end |
| AKT (Applied Knowledge Test) | Pass | 3 attempts available; discuss timing with trainer/TPD | Aim ~6 months in |
| SCA (Simulated Consultation Assessment) | Pass | 3 attempts available; practice in SCA group is essential | Aim ~6 months in |
| Compliance Passport | Annual | BLS · Defibrillator · Adult Safeguarding · Child Safeguarding (all with log entries) | Within 12 months — book early |
| Performers' List Application | 1 | Apply as GP Registrar via PCSE Online — NOT as GP Performer | Between 6 and 3 months before CCT |
| Final ESR and CSR | 1 each | All 13 PCs must reach "Competent for Licensing" — prepare carefully | Final 2 months of training |
WPBA & ePortfolio Excellence
📊 ST3 WPBA Numbers
| CATs total | 5 |
| COTs total | 7 |
| Audio-COTs (min) | 1 |
| Log entries/month | 4 |
📝 Log Entry Breakdown
CAT Types Available in ST3
In ST3 (unlike ST1/ST2), you are no longer limited to CbDs. You can combine different CAT types to reach your target of 5:
| CAT Type | What it involves | When useful |
|---|---|---|
| Case-Based Discussion (CbD) | Structured interview about a real case you managed; explores your clinical reasoning | Any point in ST3; the most familiar format |
| Random Case Review | Supervisor reviews a random selection of your consultations | Useful when you want honest, unselected feedback |
| Routine Session Review | Observer reviews a complete surgery or session | Good for overall consultation patterns |
| Referrals Review | Analysis of a selection of your referral letters and decisions | Useful when referral behaviour is a learning priority |
| Prescribing Assessment | Review of your prescribing habits with a clinical supervisor | Can double as Prescribing Review evidence |
| Duty Session Review | Review of an on-call or duty doctor session | Good for UUC / OOH experience evidence |
🎯 COT Case Selection — Go for Range, Not Comfort
Do not save only your easiest cases for COTs. A good range of case types tells a richer story to your trainer and to the ARCP panel. Aim to cover:
💡 Use CATs Strategically — Not Just as Boxes to Tick
The CAT structure is broader than traditional CbDs. Use it to showcase your professional judgement across the full scope of general practice. Specifically, use CATs to demonstrate:
- Diagnostic reasoning — how you arrived at your working diagnosis
- Safe prescribing — particularly for high-risk drugs, older adults, or polypharmacy
- Use of resources — appropriate investigations, referrals, and resource allocation
- Handling complexity — multi-morbidity, social complexity, or uncertainty
- Ethical reasoning — consent, confidentiality, capacity, best interests
- Workload and organisational thinking — how you managed competing clinical priorities
- Good safety-netting and follow-up planning — explicit, specific, documented
💡 How to write a log entry that actually impresses ARCP panels
The most common failure mode in log entries is description without reflection. "I saw a patient with chest pain and made a management plan" is not a log entry — it's a diary entry. What panels want to see is:
- What you were thinking and feeling during the encounter
- What you noticed about your own performance — the good and the less good
- What you have learned or changed as a result
- Evidence for at least one Professional Capability — named explicitly
Use the ISCE framework: Information → Self-awareness → Critical analysis → Evidence of learning. A good entry takes 15 minutes. A great entry might take 30. But it will be read by someone who doesn't know you — and it is the primary evidence of your learning across three years of training.
- A long story with no clear learning point at the end
- No discussion of clinical decision-making or reasoning
- No reflection on uncertainty, risk, or follow-up plans
- No explanation of what you would do differently next time
- Poor or absent capability linking
- Uploading many entries all at once, late in the review period
- What was difficult here?
- What clinical uncertainty was present and how did I manage it?
- What influenced my decision — guidelines, experience, patient values?
- What risk did I need to exclude?
- What communication skill mattered most in this encounter?
- What system issue affected care (positively or negatively)?
- What will I now do differently?
Consultation Development in ST3
✅ What a strong ST3 consultation looks like
- A purposeful, warm opening
- Agenda set early — including hidden agenda
- Focused but flexible data gathering
- Attention to patient cues and concerns (ICE)
- Sensible examination planning — or remote assessment where needed
- A working diagnosis or a clear uncertainty statement
- Explanation in plain English — not jargon
- A plan that is proportionate to the situation
- Explicit, specific safety-netting
- A closing check that the patient understands and agrees
❌ What a weak ST3 consultation looks like
- Diving into data gathering before building rapport
- Ignoring cues and going through a protocol instead
- Over-investigating because the diagnosis is unclear
- Explaining in medical language the patient cannot follow
- Generic safety-netting: "come back if it gets worse"
- Not involving the patient in the plan
- Closing without checking understanding or hidden concerns
- Consulting fast but unsafely
🕐 Realistic Consulting Time Target for ST3
Early in ST3, longer appointments are entirely acceptable while you are developing confidence. The realistic contemporary target by the end of ST3 is consulting at approximately 15-minute appointments safely and consistently, while managing the wider surgery workload. This is what "ready for independent practice" looks like — not the speed of the consultation alone, but the quality and safety within that time frame.
🗣 What to practise deliberately for SCA consulting
These aspects of consulting do not self-improve through clinical experience alone. They require deliberate attention:
- Explanation skills — how to structure a diagnosis explanation for a patient who has never heard the term before. Practise with your trainer. Ask: "Was that clear?"
- Empathy and acknowledgement — genuinely reflecting the patient's emotional state, not formula-phrases. "That sounds really difficult" works; "I understand your concern" is starting to sound scripted.
- Signposting — telling the patient what you're about to do before you do it: "I'd like to ask you a few questions about your symptoms, then examine you, and then we'll talk about what I think is going on — does that sound okay?"
- Shared decision-making — involving the patient genuinely, not just presenting options and waiting for a nod. "What are your thoughts on that?" is the minimum.
- Telephone consulting — the absence of visual cues changes everything. Practise specifically for this format: verbal signposting, checking understanding more frequently, building safety-netting into the verbal summary.
SCA vs AKT — At a Glance
Two very different exams requiring two very different preparation strategies. Know the difference before you plan your revision.
| Feature | AKT | SCA |
|---|---|---|
| What it tests | Clinical knowledge, evidence, organisational reasoning | Consultation performance — data gathering, management, relating to others |
| Format | ~200 MCQs (SBA, EMQ, data interpretation) — 3 hours | 12 remote simulated consultations — 12 min each + 3 min reading |
| Best prepared by | Reading NICE/CKS + question banks + 3R loop | Roleplay with feedback + full session simulation + COT debriefs |
| Biggest mistake | Relying only on question banks without reading guidance | Daily consulting without deliberate exam-focused practice |
| Key domain weighted most | Clinical medicine (~80%) | Clinical Management (spans several capability areas) |
| Physical exam | Tested in knowledge (management of findings) | NOT assessed — covered in WPBA instead |
| When to sit | ~6 months into ST3 (discuss with TPD) | ~6 months into ST3, ideally near AKT |
AKT & SCA Exam Preparation
The AKT and SCA are the two summative MRCGP exams you need to pass in ST3. Both test different things. Both require deliberate, structured preparation — not just "doing lots of GP." Here's what actually works, drawn from trainee experience and evidence on effective learning.
🔥 AKT — Applied Knowledge Test: What Actually Works
GP breadth + "must not miss"
Stats, critical appraisal
DVLA, capacity, complaints, QOF
Question formats: mostly Single Best Answer, extended matching, and data-interpretation tables/graphs — not simple recall. It is written to GP level: common problems + prescribing safety.
🎯 6 High-Yield Areas — Focus Here First
💡 Practical tip: map your tutorials and self-study to the RCGP AKT feedback reports — they list the top weak areas from recent sittings. Revise those areas first, not randomly.
⚠️ 5 Common AKT Traps — Seen Repeatedly
- Not reading the stem slowly. Candidates miss critical details: "pregnant", "breastfeeding", "eGFR 28", "known AF", "already tried sertraline". One missed word changes the answer.
- Distractor answers built from "almost right" guidelines. Old thresholds, wrong first-line drug, or a hospital-appropriate answer that is wrong in primary care — these are deliberate distractors.
- Overvaluing rare diseases when the stem is clearly describing a bread-and-butter GP presentation. If it walks like a UTI and talks like a UTI, it's probably a UTI.
- Data-interpretation: jumping to the label ("UTI", "heart failure") without checking all the numbers — CRP, BNP, HbA1c, eGFR, ECG features. Look at all the data before deciding.
- Rushing the organisational/ethics questions at the end. These are highly scorable and often straightforward if you know the principles. Don't treat them as an afterthought.
📋 AKT Study Strategy
- Register via MyRCGP. From late 2025, AKT and SCA booking moved to MyRCGP. Check current RCGP guidance for how to reserve your place through your trainee portfolio.
- Start at least 4–6 months before your exam date. Cramming 200 topics in 8 weeks does not work. Spaced repetition over months does.
- Read proper guidance — not just question banks. NICE CKS, BNF, and RCGP curriculum documents are the primary sources. Use question banks to test and consolidate — not as your only source.
- Do little and often rather than irregular panic bursts. In the final month, aim for 1–2 timed blocks (e.g. 50 questions) most days, with full review of wrong answers.
- Use the 3R loop for each topic: Read one trusted guideline → Respond to 10–20 questions on that topic → Review by writing down 3–5 key thresholds and 1 "typical trap." Repeat across curriculum domains; revisit weak areas before exam.
- Use RCGP self-tests in the final 3–4 weeks to tune your ear to actual AKT wording — different from commercial question banks in style.
- Know the common number-based traps: drug monitoring intervals, antibiotic durations, screening programme criteria, cancer referral thresholds (2WW), guideline numbers (HbA1c targets, BP thresholds, QRISK cut-offs).
- Don't neglect the ethics/organisational 10%. DVLA fitness to drive, GMC Good Medical Practice, notification duties, controlled drugs, capacity, consent — very learnable and often straightforward marks.
🎯 SCA — Simulated Consultation Assessment: What Actually Works
remote simulated consultations
12 consult + 3 reading time
across 3 domains
- Data Gathering & Diagnosis — focused history, red flags, working diagnosis
- Clinical Management — weighted more than the other two; spans several capability areas including safety-netting, referral, prescribing
- Relating to Others — empathy, ICE, explanation, shared decision-making
⚠️ Physical examination is NOT assessed in the SCA. It is covered in WPBA. You must show safe management based on history, probability, and remote assessment alone.
✅ What Examiners Explicitly Say They Are Looking For
- Efficient, focused history taking — not a generic systems review from start to finish
- Ability to handle uncertainty and use probability language ("most likely", "we also have to exclude")
- Clear explanation of options, then making a decision with the patient — not endless hedging
- Concrete safety-netting — what to watch for, how and when to re-contact
- Flexibility — adapting to patient concerns rather than rigidly following a script
😤 6 Behaviours That Irritate Examiners
- Not listening or responding to what the patient actually said — going through your own agenda instead
- Wooden, checklist-like ICE questions ("Any ideas? Concerns? Expectations?") with no follow-up on what the patient actually answers
- Overlong history with little or rushed management — spending 9 minutes on history and 1 minute on the plan
- "Lecturing" the patient — reciting NICE guidance rather than tailoring key bits to this specific patient
- Vague or generic safety-netting — "come back if worse" with no specific symptoms, timeframe, or route
- Asking questions already given in the written brief — wasting time and showing you didn't read the preparation material
💡 What Successful Candidates Say (Trainee Community Insights)
- Practising with another person is the single strongest predictor of improvement. Use good casebooks or SCA-style websites to structure sessions by theme.
- Simulate full 12-case sessions with breaks — this builds stamina and exposes pacing problems early.
- Treat every real-life surgery as SCA practice — time yourself, write brief "debrief" notes after tricky consultations ("what was my diagnosis? did I say it out loud? was my safety-netting specific?").
- Deliberately seek exposure to: vulnerable adults, safeguarding, professional conversations, and undifferentiated new presentations — not just straightforward single-problem cases.
- Remember: daily consulting does NOT automatically equal exam-ready consulting. The SCA tests a specific structured performance. Deliberate roleplay with feedback is essential.
- Explanation, empathy, signposting, and shared decision-making need deliberate practice — they do not self-improve.
- Under-prepare for telephone consultations at your peril — speaking too quickly, not checking understanding, poor signposting on the phone costs marks.
🗣 SCA Consultation Phrases — Ready for Use Tomorrow
These phrases are designed to sound natural, not scripted. Read them once. Use them. Adapt them to your own voice.
- "How can I help you today?"
- "I've read the note — it would help if you could tell me in your own words what's been going on."
- "Hello, I'm Dr [Name]. How would you like me to address you?"
- 📞 On the phone: "You're through to Dr [Name] at [practice]. Is it still okay to talk now, and are you somewhere private?"
- "What's your sense of what might be going on?"
- "Is there anything in particular you're worried this could be?"
- "What were you hoping we might do for you today?"
- "How has this been affecting your day-to-day life?"
- 🎯 Follow-up (this is where marks are scored):
"You mentioned you were worried about cancer — can you tell me what led you to that?"
"You were hoping for some tests; let me explain what we can do today so we're on the same page."
- "That sounds really difficult."
- "Take your time — there's no rush."
- "It makes complete sense that you're concerned."
- 🎯 Interpretive (higher scoring):
- "Given everything else you've got on at the moment, I can see why this has been really draining."
- "It sounds like you've been carrying this on your own for a long time."
- "You've done really well to manage this for so long before asking for help."
- "From what you've told me, the most likely explanation is [X]."
- "There are a couple of other possibilities we should bear in mind, such as [Y], but there's nothing currently to suggest anything more serious like [Z]."
- "Medicine is rarely black and white — at the moment the balance of probability is that this is [X]."
- "I want to be honest with you — I'm not entirely certain yet. Here's what I'd like to do to find out."
- "There are a few reasonable options — I'll run through them, and then we can decide together what feels right for you."
- "Option one is [brief], which might suit you if [context]. Option two is [brief], which has the advantage of [benefit] but the downside of [risk]."
- "Based on what you've told me about [ICE], my suggestion would be [X]. How does that sound?"
- "What matters most to you in how we manage this?"
- Specific: "If you notice any of the following, seek help urgently: chest pain that doesn't go away, struggling to breathe, feeling faint or confused, or pain suddenly much worse."
- Explain WHY: "Because problems can change over time, I always give a clear plan for what to watch out for."
- Clarify WHO acts: "If you notice these changes, I'd like you — or your family — to contact us or NHS 111 straight away."
- Teach-back: "Just so I know I've explained it clearly — what will you be looking out for over the next few days?"
- Check acceptance: "Does that plan feel clear and doable for you?"
- "We've talked about [diagnosis], [treatment], and what to look out for. Is there anything important you feel we haven't covered today?"
- "Just to recap — you're going to [action], and we'll [follow-up plan]. If things change sooner, you know how to get back in touch."
- "Does that all make sense?"
- "Do you feel happy with the plan we've agreed?"
📋 Two Adaptable Consultation Templates
e.g. chest discomfort, rash, cough
- Opening + agenda: "Tell me in your own words what's been happening and what you were hoping I could help with today."
- Focused SOCRATES + key red flags + brief background (PMH, DH, FH where relevant)
- Check ICE early — and revisit it later
- Signpost: "I've got a good picture now; let me explain what I think is going on and we can agree a plan."
- Explain likely diagnosis + rule-out of serious condition with probability language
- Offer options; decide together
- Safety-net with specific triggers, timeframe, and route
- Check understanding and close
e.g. diabetic with new symptom, elderly with multiple problems
- Agenda setting: "You've mentioned [new symptom] and you also live with [conditions]. We've got about 12 minutes — which feels most urgent for you today?"
- Focused history on priority issue + quick screen for interaction with existing conditions/medications
- ICE around both the new problem and long-term concerns
- Acknowledge complexity: "You've got a lot going on — let's focus on [priority] today and make a plan to address [secondary issues] in follow-up."
- Explain working diagnosis and how it sits within multimorbidity
- Agree pragmatic plan: small changes, realistic goals, appropriate follow-up
- Targeted safety-netting — for both the acute and background conditions
- Arranged follow-up and verbal summary
GP 7-Step Practical Framework
Use this 7-step approach consistently in your ST3 clinics. It aligns naturally with SCA expectations and generates real cases that reinforce your AKT knowledge. Practise it deliberately until it becomes automatic.
- Establish rapport quickly; confirm identity; check if now is a good time (especially phone/video)
- Get a concise opening statement — then set an agenda, especially with multiple problems
- On the phone: "You're through to Dr [Name]. Is it okay to talk now, and are you somewhere private?"
- Ask targeted red-flag questions guided by the presenting symptom (e.g. for headache: neuro signs, meningism, thunderclap onset)
- Be explicit with patients when ruling out serious diagnoses — this both reassures and demonstrates safe practice to an examiner
- In children with fever: breathing difficulty, non-blanching rash, reduced responsiveness, poor feeding, persistent fever ≥5 days
- Explore impact on function: sleep, work, caring responsibilities
- Weave in relevant comorbidities and high-risk drugs (steroids, anticoagulants, immunosuppressants)
- Understand psychosocial context: who is at home, caring responsibilities, financial/work stress, safeguarding concerns
- Use plain language and metaphors where helpful — avoid jargon
- Name the working diagnosis and the degree of certainty: "The most likely cause is X, though we also need to consider Y"
- Explain why you are (or are not) ordering tests — don't leave patients guessing
- Offer realistic options: self-care, community interventions, medication, watchful waiting, referral
- Include lifestyle and psychosocial support — not only prescriptions
- Make a decision with the patient and summarise: "We've agreed that…"
- Spell out symptoms and timeframes that should trigger re-contact, and which route (practice / 111 / 999)
- Check understanding: use teach-back — "Just so I know I've explained it clearly — what will you be looking out for over the next few days?"
- Not documenting or verbalising safety-netting is seen as unsafe in both real practice and SCA
- Decide explicitly whether and when to review: face-to-face, phone, nurse vs GP
- For referrals: explain what the service does and rough timescales; tell the patient what to do if they haven't heard by a certain date
- Arrange follow-up proportionate to the clinical risk — not "routine" for everything
Common Pitfalls — Things That Catch Trainees Out
-
Leaving all WPBAs to the last 2 months. This is the most common ST3 mistake. It results in poor-quality rushed assessments, stressed trainees, and trainers who are (politely) disappointed. Start month 2. One CAT or COT every 4–6 weeks.
-
Forgetting to apply to the Performers' List. Every year, trainees reach CCT and realise too late. You cannot practise as an independent GP without being on the list. Apply between 6 and 3 months before CCT — as a GP Registrar, not a GP Performer.
-
ePortfolio entries that are all description and no reflection. "I saw a patient with X and did Y" is a diary entry, not a learning log. ARCP panels need to see that you learned something — specifically, and with evidence. Use the ISCE framework every time.
-
Starting AKT revision too late. Three weeks of cramming does not substitute for four months of spaced practice. The AKT covers vast breadth. Start early. Use active recall, not re-reading. Join a study group.
-
Preparing for SCA alone. SCA is a performance exam. If you only ever practise alone or in your head, you will find the real exam experience jarring. Practise with peers, with your trainer, with anyone willing to role-play as a patient.
-
Treating the Leadership Project as an afterthought. It is mandatory. It takes time. Start it in months 3–6 when the exam pressure is lower. Don't pick something enormous — a small, well-evidenced project done properly impresses more than a grand ambition abandoned halfway.
-
Leaving all OOH sessions to the final stretch. Not only stressful — it also shows poor time management to your ARCP panel. Spread UUC experience throughout the year.
-
Not reading a consultation book. Most trainees read clinical revision resources. Far fewer actually read a consultation book. The ones who do have more natural, flexible consultations — and they score better in SCA.
-
Generic or absent safety-netting. "Come back if worse" is not safety-netting — it is a liability. In both real practice and SCA, safety-netting must be specific (named symptoms), timed, and route-specified. Not documenting it is seen as unsafe practice.
-
Missing safeguarding and capacity cues. Ignoring safeguarding concerns or failing to explore them is both an exam failure and a real-world risk. If inconsistencies or concerns are present — explore them, even briefly. Dismissing concerns without explaining your reasoning ("it's just viral") is clinically and medico-legally risky.
-
Neglecting organisational and ethics topics in AKT prep. Capacity, consent, DVLA, complaints, significant event analysis, controlled drugs — these make up 10% of the AKT and are highly learnable. Many trainees leave them until last or skip them entirely. These are easy marks if you prepare.
-
Over-formal or didactic consulting style (especially IMGs). UK patients and examiners expect a conversational, collaborative style — not a formal lecture. "Lecturing" — reciting NICE guidance rather than tailoring it to the patient — is one of the most commonly cited examiner irritants.
-
Focusing on "covering everything" instead of prioritising. In a 12-minute SCA case (or a 15-minute real consultation), you cannot cover everything. Prioritise what matters most, signpost what you are leaving for another time, and do the most important things well.
-
Ignoring your wellbeing. ST3 is intense. Trainees who grind through without looking after themselves make more mistakes, perform worse in exams, and are less pleasant to work with. Your wellbeing is not a luxury — it is a patient safety issue.
Insider Pearls — What Nobody Quite Tells You
High-yield non-official insights drawn from trainee experience, examiner feedback, and real GP training communities.
🤔 4 Reflective Questions — Ask Yourself Weekly
These questions are uncomfortable if you answer them honestly. That discomfort is the feeling of learning happening.
- 💬 "In my last clinic — which consultation would probably have failed the SCA, and why?"
- 💬 "When did I last explicitly use probability language with a patient? ('The most likely cause is…', 'We also need to exclude…')"
- 💬 "How often do I safety-net with specific triggers, timeframes, and actions — or do I still say 'come back if worse'?"
- 💬 "What AKT topics keep appearing in my wrong answers — and what specifically will I do about that this week?"
For Trainers & TPDs — Teaching Pearls
Common ST3 Learner Blind Spots
These are the areas where ST3 trainees most commonly need deliberate teaching input — things that don't self-correct through clinical experience alone:
- Underestimating the ePortfolio — trainees often write log entries quickly without genuine reflection. A 15-minute tutorial on what "good" looks like transforms entry quality overnight.
- WPBA procrastination — the trainee assumes you will remind them. Explicitly clarifying that this is their responsibility — and why — usually resolves this early.
- Consultation efficiency plateau — trainees sometimes plateau at 15 minutes after becoming comfortable at that pace. A specific focus on consultation structure and active debriefs can shift this.
- ICE as a scripted box to tick — trainees who don't understand ICE at a deeper level use it formulaically, which patients and examiners notice immediately. Teach the purpose of ICE, not just the phrases.
- Leadership Project avoidance — often left too late. Identifying it as a month 3–4 task in the placement planning meeting and reviewing progress at mid-year ESR prevents the typical month-10 panic.
💬 Tutorial ideas and discussion prompts for ST3 trainees
These work well in one-to-one tutorials and can generate rich reflective conversations:
- "Tell me about a consultation this week where you surprised yourself — good or bad."
- "If you had to describe your consultation style to someone who'd never seen you consult — what would you say?"
- "What does good safety-netting actually sound like? Let's practise it."
- "Walk me through how you prepare for an Educational Supervision meeting — what's your approach?"
- "Which of the 13 Professional Capabilities do you find hardest to demonstrate evidence for — and why?"
- "Tell me about a time this month when you were uncertain. What did you do with that uncertainty?"
- "If you were sitting the SCA tomorrow, what would be your biggest worry? Let's address it."
- "What has your Leadership Project taught you about yourself as a doctor, not just as a project manager?"
🎭 3 Teaching Case Scenarios — Ready to Use in Tutorials
These structured scenarios work well for peer groups, one-to-one tutorials, and SCA roleplay sessions.
Role-player: Parent of a 2-year-old with fever, calling for remote triage advice.
Candidate tasks: Focused remote assessment; verbal safety-netting aligned with NICE fever in under-5s (urgency indicators, red flags, home care advice).
Debrief question: Did the trainee explain why they were safety-netting, and who should act if the child deteriorates? Was the safety-netting specific or generic?
Role-player: A GP colleague asking for advice about a patient with a borderline PSA result who is very anxious about cancer.
Candidate tasks: Explore concerns; balance over- vs under-investigation; support a shared decision about referral; document a clear plan.
Debrief question: Did the trainee use probability language? Did they address the patient's anxiety alongside the clinical question?
Format: Trainer brings 3–5 anonymised cases with relevant guideline thresholds. Trainee must choose the best AKT-style answer and explain why the other options are wrong.
Teaching goal: Reinforce that AKT tests application, not recall. "Why is option B wrong?" is more educational than "what is the correct answer?"
Variation: Ask trainee to bring "three numbers I learnt this week" and test how to use them in a case scenario rather than just recall them in isolation.
📚 How to assess learning on the Four Pillars in a tutorial
Each pillar lends itself to a different type of tutorial activity:
| Pillar | Best tutorial activity |
|---|---|
| Relationships | COT review with specific micro-skill focus (ICE, empathy, explanation quality). Role-play of a difficult consultation. |
| Decision-Making | Random case debrief. CBD preparation and discussion. Clinical scenario "what would you do?" exploration. |
| Management | Review of a week's administrative challenges. Discussion of the trainee's daily work routine. Observation of computer use during a consultation. |
| Professionalism | Review of a log entry together. Discussion of a challenging patient or team interaction. Feedback on MSF results. |
Memory Aids & Cheat Sheets
🏛 RDMp — The Four Pillars
📝 ISCE — Log Entry Framework
🩺 CARE PLAN — SCA Consultation Framework
🎯 SMART — PDP Goals
🛡 Safety-Netting Checklist — 4 Points (BMJ Framework)
Before finishing any consultation, check you have:
- What to look out for — specific symptoms or time-course
- Why you are giving this advice ("problems can change")
- Who should act and how — phone practice / 111 / 999
- Patient understands and accepts — use teach-back: "Just so I know I've explained it clearly — what will you be looking out for?"
🔢 ST3 Numbers to Remember
Practical ST3 Survival Advice
The stuff trainees often wish they had taken seriously a bit earlier. Strongly echoed across trainee discussion threads about AKT, SCA, ST3 stress, and portfolio pressure.
A Simple ST3 Year Plan
Use this alongside the detailed phased roadmap above. The right move is not "work harder later" — it is "start earlier and spread it better."
| Phase | Focus | Key tasks |
|---|---|---|
| First month | Settle in properly | Understand systems, supervision, appointments, portfolio access, tutorials, and PDPs. Identify obvious weak clinical areas now. |
| Months 1–3 | Set the year up | Start regular logs, begin COTs and CATs, plan courses, identify weak areas, start exam preparation, arrange regular MSF, draft year plan for all mandatory items. |
| Months 4–6 | Build momentum | Keep assessments moving, continue exam preparation, review portfolio range, do not let UUC drift, mid-year ESR. Aim to attempt AKT/SCA around this period if on track. |
| Months 6–9 | Complete and consolidate | Complete leadership activity, organise leadership MSF, do PSQ and prescribing review if not already done, keep building evidence for final ESR, complete remaining COTs/CATs. |
| Last 3 months | Final readiness | Check every mandatory item, review evidence quality not just quantity, prepare for final ESR and ARCP, sort Performers' List timing, think about career next steps. |
The Performers' List — Apply Before You Qualify
The Performers' List is a register managed by PCSE (Primary Care Support England) confirming that a GP is qualified, vetted, and cleared to work independently in NHS primary care. In England, there is one National Performers' List. Scotland, Wales, and Northern Ireland have their own processes.
Application Timeline
Log into PCSE Online and begin your application. Select GP Registrar (not GP Performer). Start gathering your documents now.
Your application must be submitted by this date. Processing takes time. Late applications may delay your ability to work after qualification.
Once you have your CCT, log into PCSE Online and update your status from GP Registrar to GP Performer. This is a simple change — but you must remember to do it.
📄 Documents needed for the Performers' List application
- Enhanced DBS certificate (or DBS tracking reference if certificate not yet received)
- Police check certificate (if you have lived or worked abroad in the last 5 years)
- Full CV with employment history from graduation date — explain any gaps
- Photo ID (passport or driving licence)
- Graduation certificate
- Scanned copy of your signature
- Appraisal information if applicable
PCSE frequently return applications because of missing or incorrect information. Get your documents together early and check them against the application guide before submitting.
PCSE Performers' List (England) →🔍 Performers' List — FAQ
Yes — search the Performers List for England online. Some trainees were added during the pandemic period.
You apply to the relevant local Health Board. Entry to one HB list includes all other HB lists across Scotland.
Apply to the Wales Performers List via the Primary Care Services Wales website.
Apply through the HSC Business Services Organisation.
Separate to the Performers' List. You also need to be on the GMC's GP Register. GMC GP Registration →
Final Take-Home Points — The Bits to Remember Tomorrow
The Bottom Line — 10 Things Worth Taking Away
- ST3 is one year, not twelve months. Start with the end in mind. Know your mandatory requirements from day one.
- WPBAs spread throughout the year are always better than a sprint at the end. Always. No exceptions.
- Your ePortfolio speaks for you when you're not in the room. Write log entries that reflect genuine learning — not waffle to tick a box.
- AKT preparation requires months, not weeks. Active recall and question banks beat re-reading. Spaced practice beats cramming. Start early.
- SCA requires performance practice, not just knowledge. You cannot get better at being observed without being observed. Find a study group. Do real cases.
- Apply to the Performers' List between 6 and 3 months before CCT. As GP Registrar. Via PCSE Online. This is not optional.
- The Leadership Project is mandatory and takes more time than you think. Start it in months 3–6. Keep it small and well-executed.
- Your wellbeing is a clinical safety issue. Tired, stressed doctors make more mistakes. Looking after yourself is part of being a good doctor.
- If you are an IMG — start working on your English now, not later. The SCA is language-dependent. Immersion is the only approach that works.
- You are closer to being ready than you feel. Nearly every trainee approaching CCT feels unprepared. Most of them pass. You have been building towards this for three years. Trust it.
"The best ST3 trainees are not the ones who know everything.
They're the ones who know what they don't know — and go looking for it."
— Bradford VTS Philosophy