Hospital Training Roadmap
ST1 & ST2
Hospital posts are where you earn your GP stripes — if you know what to focus on. Here's your six-month survival and success guide.
Your hospital posts are not a detour from GP training — they are a foundation. Every ward round, every clerk-in, every difficult conversation is building the doctor you will become. This page tells you exactly what to focus on, when, and why it matters.
Last updated: April 2026 | by Dr Ramesh Mehay
Web Resources
A hand-picked mix of official guidance and real-world GP training resources — because sometimes the best pearls are not hiding in the official documents.
📋 Core GP Training Guidance
- RCGP GP Specialty Training Curriculum — The official framework you are being trained against
- RCGP WPBA Guidance — Official word on all workplace-based assessments
- FourteenFish ePortfolio — Log in regularly; don't leave entries to the last minute
- NHS England GP Training — National training requirements and structure
🏥 Hospital Post Essentials
- Bradford VTS: Hospital Post Induction — What to do on day one
- Bradford VTS: Comm Skills in Hospital — How to use hospital posts for SCA prep
- Bradford VTS: CEPS Guide — Get these done in hospital, not GP
- Bradford VTS: Mini-CEX Guide — Hospital assessment — everything you need to know
📚 ePortfolio & Assessments
- Bradford VTS: Learning Log Entries — How to write entries that actually impress ARCP panels
- Ram's Easy Peasy Log Method — The shortcut to writing brilliant log entries
- Bradford VTS: CBD Resources — Full guide to Case-Based Discussions
- Bradford VTS: Educational Supervision — How to prepare for your ES meetings
🌱 Development & Wellbeing
- Bradford VTS: Professional Capabilities — The 13 things you are measured against throughout training
- Bradford VTS: How to Study Effectively — Research-backed study methods worth adopting now
- Bradford VTS: QI Projects — Everything on quality improvement — do this in ST1
- Bradford VTS: Writing Your PDP — SMART PDPs that your trainer will actually appreciate
- Bradford VTS: Community Placements — Making the most of non-hospital placements too
Quick Summary
If you only read one section — let it be this one. Everything else is the detail behind these points.
🎯 The Hospital Post in 10 Bullets
- You are a GP trainee in a hospital — never forget that. Focus on what will serve you in GP practice, not just on the specialty you're in.
- Hospital posts are your golden opportunity to nail CEPS (clinical examination and procedural skills) and mini-CEXs — these are harder to do in GP land.
- Each 6-month hospital post requires a minimum of 2 × mini-CEXs and 2 × CBDs. Don't do them all in the last two weeks.
- The 4 pillars of every hospital post: Relationships, Decision-Making, Management, and Professionalism. Think about all four from day one.
- Write one learning log entry per week — 3 clinical, 1 other. Do this consistently and your ARCP will thank you.
- You must do a QI (Quality Improvement) project before the end of ST1. Start thinking about it early — it needs more time than you think.
- Get to know the nurses, healthcare assistants, ward clerks, and everyone else on the team. They will save you more than once. The doctor is not the top of the hierarchy — everyone matters.
- Read a consultation skills book during hospital posts. Your 10-minute GP consultations will be here before you know it.
- If your English fluency needs work, start now. ST1 is your biggest window. By ST3, you'll have exams, and there won't be time.
- Your ePortfolio is your professional story. Write it carefully — the ARCP panel may not know you, and they will judge you entirely on what they read.
Why Hospital Posts Matter for GP Training
Hospital posts are not a necessary inconvenience on the way to becoming a GP. They are where several of the most important foundations are built.
Clinical Depth
Hospital posts give you exposure to acute illness, rare presentations, and clinical complexity you simply won't see at the same volume in general practice. That depth matters.
Examination Skills
CEPS — your mandatory clinical examination competences — are best completed in hospital. Examiners, equipment, and variety of presentations are all on your doorstep.
Communication Under Pressure
Breaking bad news. Managing angry relatives. Urgent ward conversations. These are skills you can practise and hone now — and they translate directly to the SCA in ST3.
Teamwork & Hierarchy
You will work in large, diverse MDTs. Learning to communicate across roles — with nurses, porters, physios, consultants — is a core professional skill for any GP.
Systems & Processes
Hospital computer systems, referral pathways, discharge letters, result management — understanding how hospitals work makes you a better GP when interpreting letters and managing patients.
GP-Relevant Clinical Filtering
In O&G, learn HMB management — not just how to assist at caesareans. In respiratory, learn COPD management — not just bronchoscopy technique. Think GP all the way through.
💬 What Trainees Wish They Knew Before Starting
Four hard-won insights from GP trainees who have been through hospital posts. Read them now — not in month five.
"Hospital posts are where you deliver a service.
GP training is what you extract from them."
Trainee consensus — UK GP forums
Hospital posts are service delivery. GP learning is what you actively extract.
You will not automatically learn GP medicine by being in a hospital. The learning happens when you deliberately filter every case through a primary care lens. Nobody will do this for you.
The GP Lens Filter — apply after every case
💡 The 3 questions to ask yourself after every case tap to open
You may be on-call from week one. Shadow before your official start if possible.
Most hospitals will accommodate shadowing before your first official shift. Do it. Being thrown onto an on-call rota having never seen the ward layout, computer systems, or escalation procedures is avoidable — and stressful.
Before your first day — a simple action timeline
Ask if you can shadow for 1–2 days before your start date. Most hospitals say yes.
Contact your consultant: "I'm a GP trainee — I need X mini-CEXs and CBDs. Can I flag when I'd like one done?"
Know crash trolley, fire exits, IT login, escalation procedure before you see your first patient.
The ePortfolio minimum is 36 clinical case reviews per year. Hospital reflections need a different approach.
Hospital log entries are harder than GP ones because consultants make most decisions — and trainees can feel like they "didn't do anything." The trick is reflecting on your own thinking, not just on the outcome.
per year minimum
= on target
= exceeding
🔺 The Hospital Reflection Triangle — when the consultant made the decision tap to open
IMGs: Communication IS clinical competence in UK GP. This is the biggest shift to make.
In many health systems around the world, clinical knowledge and technical skill are the primary currency of a good doctor. In UK general practice, interpersonal and communication skills are clinical competence — not a soft extra on top.
How clinical competence is weighted — a perspective shift
These figures are illustrative approximations to convey the conceptual shift — not official statistics. The SCA exam dedicates one full domain to "Relating to Others." It is not a soft add-on; it is a third of the marks.
🧠 Quick self-check — are you making the most of your hospital post? tap to open
Honest yes/no. If you answer no to more than two, reread this section.
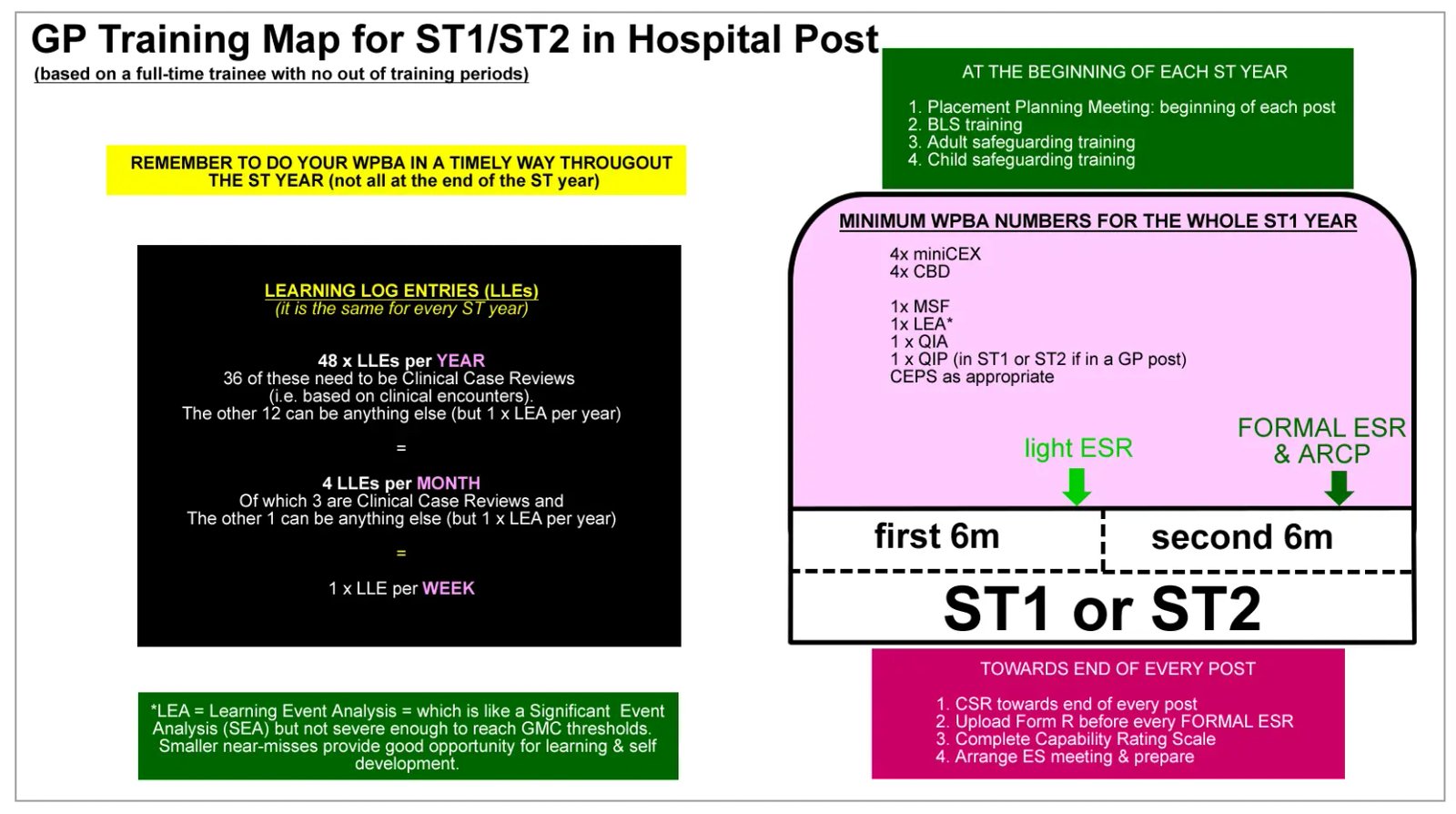
The ST1 / ST2 Hospital Training Map
A visual overview of what you are working towards across each hospital placement.
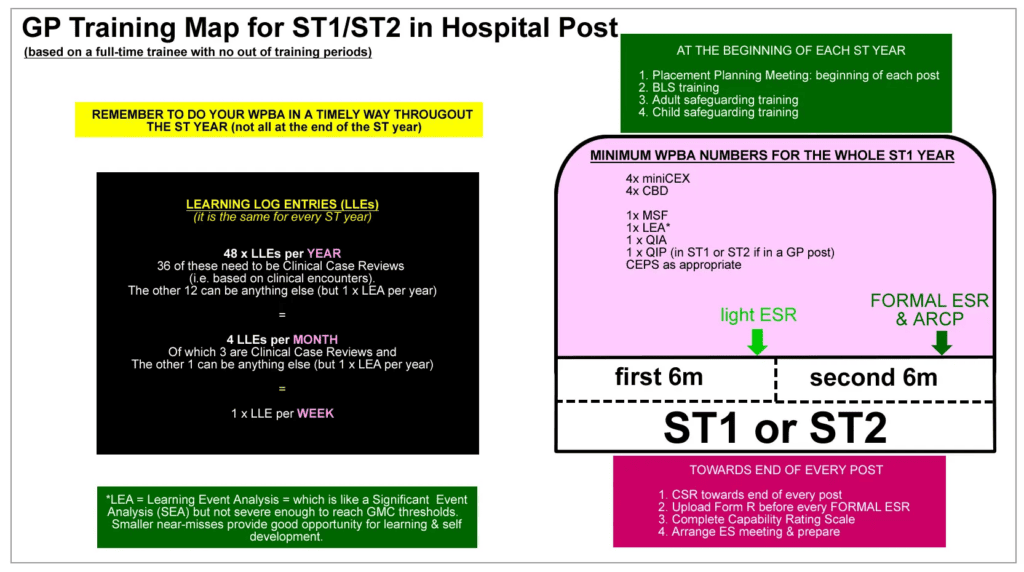
Mini-CEXs are done in hospital posts only. COTs (Consultation Observation Tools) are done in GP posts only. If your ST2 year is split — 6 months GP, 6 months hospital — you will need 4 × CBDs, 2 × COTs, and 2 × mini-CEXs by the end of that year. If the whole of ST2 is hospital posts, it is 4 × CBDs and 4 × mini-CEXs.
The 4 Pillars of Every Hospital Post
Everything a hospital placement can teach you — and everything you will be assessed on — falls into one of these four areas. Think about all four from day one. Use them to plan your Placement Planning Meeting too.
Relationships
Consulting with patients, working with diverse teams, presenting cases, breaking bad news, managing difficult conversations. The communication skills you build here are the raw material for your SCA exam.
Decision-Making
Clinical reasoning, differential diagnosis, investigations, management plans, knowing your limits and when to call for help. Think: "Why am I doing this?" — not just "What am I doing?"
Management
Managing your workload, your time, your admin, your own wellbeing. Happy, organised doctors make fewer mistakes and better decisions. This pillar supports all the others.
Professionalism
Respecting patients, colleagues, contractual duties, and the ePortfolio. It underpins the other three. Professionalism is demonstrated in small acts every single day — not just in formal assessments.
At the start of each hospital post, sit down with your GP trainer or clinical supervisor and discuss what you want to develop in each of these four areas. This frames your learning intentionally — and it shows professionalism and self-awareness right from day one.
What Each Pillar Looks Like in Practice
🤝 Relationships — what "achieving" looks like ▾
What to aim for by end of placement:
- Good rapport with most patients — actively exploring their Ideas, Concerns and Expectations (ICE)
- Able to break bad news with care and structure
- Able to manage angry or distressed patients/relatives without losing composure
- Concise, structured, logical patient presentations to seniors
- Good handover skills — clear, safe, appropriately detailed
- Strong working relationships with all staff — not just doctors. Nurses, HCAs, ward clerks, physios, pharmacists
Doctors are not the most important people on the ward team — they are one cog in a system that needs every cog. Ward sisters often know protocols better than the FY1s. Get to know them. Ask them to help you. In return, they will have your back in ways that matter. Coming from a background where hierarchies are more rigid? This is one of the most important resets to make early.
Evidence to look for in your portfolio:
- Mini-CEX: Achieving Communication and Consultation Skills
- CBD: Achieving Working with Colleagues and in Teams
- MSF: Positive comments about relationships and teamwork
- CSR: Comments on good consulting and handling difficult situations
- Log entries: Reflection on specific communication micro-skills — ICE, PSO (psycho-social-occupational impact), Signposting, Screening, Setting Agendas, Summarising, Explanations, Breaking Bad News, Handling Angry Patients/Relatives, and Handling Difficult People
- Log entries show good levels of reflection on feelings — of yourself and of others
- Log entries show an appreciation for colleagues and patients as individuals
🧠 Decision-Making — what "achieving" looks like ▾
What to aim for by end of placement:
- Managing most patient presentations adequately, with gradually decreasing reliance on seniors
- Making good working diagnoses for the specialty
- Strong differential diagnosis thinking for common presentations
- Knowing where to look for information when uncertain
- Knowing your clinical limits — and when to call for help
- Able to prioritise patients by clinical urgency
There is a difference between healthy growing confidence and dangerous over-confidence. Trainees who stop seeking advice too early put patients at risk. Your supervisor should be watching for this — and so should you.
Evidence to look for in your portfolio:
- Mini-CEX: Achieving Clinical Assessment and Judgement; Clinical Management
- CBD: Achieving Data Gathering, Making Diagnoses, Clinical Management
- Log entries: Demonstrating clinical reasoning, not just describing what happened
📋 Management — what "achieving" looks like ▾
What to aim for by end of placement:
- Understands clinical and non-clinical systems in the department
- Prioritises own daily workload reliably
- Admin done on time — prescriptions, referrals, discharge letters, test results, GP contact
- Engaged in own learning and development
- Recognises when stressed or unwell and acts on it
- Attends mandatory training: BLS, ALS, safeguarding, defibrillator
Evidence to look for in your portfolio:
- Mini-CEX: Achieving Organisation & Efficiency
- MSF: No concerns over admin or task management; colleagues describe a committed learner
- ePortfolio: Timely log entries; PDP items progressed; regular engagement
⭐ Professionalism — what "achieving" looks like ▾
What to aim for by end of placement:
- Genuine respect for every person encountered — patients and all colleagues
- Shows respect for contractual responsibilities — punctual, reliable, doesn't shirk
- Responds constructively to negative feedback (this is harder than it sounds!)
- Engages with ePortfolio and WPBA meaningfully — not just to tick boxes
- Does not falsely alter medical records. (Everything has an audit trail — timestamps, changes, everything.)
All hospital and GP systems carry a full audit trail. Every word changed, every timestamp, every deletion is recorded. Adding a retrospective note is acceptable — altering the original is not. This is a disciplinary and medicolegal issue. Never do it.
At ST1/ST2 level, this is still developing — and that's expected. But start building the habit of not ordering every investigation under the sun. Begin considering the costs and effectiveness of tests and medications, even if your thinking here is not yet fully polished. GPs are the gatekeepers of NHS resources. That awareness starts now.
Evidence to look for in your portfolio:
- Mini-CEX: Achieving Professionalism
- CBD: Progressing in Ethical Approach and Fitness to Practise
- MSF: Positive comments about professionalism and attitude
What to Do and When
Each hospital post is six months. Here is your structured guide — broken into the three phases that shape every placement.
The First 4 Weeks — Get Oriented
The settling-in phase. Prioritise orientation, relationships, and understanding your environment.
📖 Understand the Professional Capabilities ▾
The 13 Professional Capabilities (PCs) are the framework you are measured against throughout training. Nearly everything you do in GP training maps to one or more of them. The sooner you understand them, the more intentionally you can gather evidence.
Don't just read the list — understand what each one actually means in practice. Think about which ones your current post is going to give you the most opportunity to develop.
📝 Understand Learning Log Entries — before you write one ▾
The single biggest mistake trainees make is diving straight into writing log entries without understanding what good ones look like. ARCP panels read hundreds of logs. They can immediately spot the thoughtful ones from the waffle.
A good log entry does three things:
- Shows evidence of the 13 PCs — it demonstrates professional capability, not just clinical activity
- Shows genuine reflection — not just "what happened" but "what I learned about myself"
- Shows evidence of learning — what will you do differently next time?
Use the ISCE method: Information (what happened), Self-awareness (how it made you feel and think), Critical analysis (making sense of it), Evidence of learning (what changes).
→ Bradford VTS: Learning Log Entries
→ Ram's Easy Peasy Log Writing Method
💭 Understand Reflection — the theory first ▾
Learning cannot happen without reflection. Most of us were never formally taught how to reflect — and then we're expected to do it in our ePortfolio.
Before writing any logs, take an hour to understand what reflection actually is. This will transform the quality of every log entry you write — not just now, but for the rest of your training.
🎓 Attend Your Scheme's Induction ▾
Your GP Training Scheme's induction is one of the most important events of your training — and one of the most frequently missed. Do not let this happen.
- Find out the date immediately — email your GP scheme administrator now
- Book it as study leave with your current post as soon as you have the date
- In a hospital post: contact the Rota Co-ordinator and your Clinical Supervisor
This induction gives you the big picture of your training journey — all the requirements, timelines, and local structures — in one place. You will not regret attending.
🤝 Meet Everyone on the Ward Team ▾
This is more important than most trainees realise. In a hospital ward, you are part of a team. The doctor is not at the top of this team — you are all interconnected, like cog-wheels. Some bigger, some smaller, but all essential.
Get to know:
- Nurses — they know protocols like the back of their hands and will keep you out of trouble
- Healthcare assistants (HCAs) — often the first to notice when a patient deteriorates
- Ward clerks — invaluable navigators of the admin labyrinth
- Your registrar and consultant — build a genuine working relationship, not just a hierarchical one
- Physiotherapists, pharmacists, OTs — you will be liaising with them regularly
The trainees who thrive in hospital posts are invariably those who make friends with the ward sister in week one. She will help you understand the protocols, give you the benefit of the doubt when you make mistakes, and tell you what you need to know before anyone else does. The doctor who ignores non-medical staff misses this entirely — and usually has a harder time.
🗺️ Get Familiar with the Ward Environment ▾
Know your physical environment before you need it urgently:
- Where are blood forms, blood bottles, IV equipment, drains?
- Where is the crash trolley? What is the crash team call procedure?
- Where is the quiet room for focused tasks (e.g. prescribing)?
- What is the spill procedure? Where is the mop and disinfectant?
- Know your fire exit procedure
- Where are physical notes kept? Is there a tablet/computer for ward rounds?
📅 Define Your Daily Work Routine ▾
Without a routine, you will miss things. Missing things in clinical medicine has consequences. Speak to the doctor you are replacing and then discuss with your registrar/consultant. Build a system that covers:
- Ward rounds — schedule and your role
- Departmental teaching times and MDT meetings
- On-call rota — how it works and your responsibilities
- Ordering bloods — do you do them or does the phlebotomist?
- Retrieving and acting on blood results daily
- Prescribing workflow and sign-off
- Computer system — who shows you the basics?
- Physical pigeon hole — check it regularly
- Email — check daily for updates and actions
- Capturing and completing clinical tasks from ward rounds
💻 Get Familiar with the Hospital Computer System ▾
Ask a colleague to show you the hospital EHR system (e.g. Cerner, EMIS, Lorenzo) on your first day. Focus on: writing a clerk-in, prescribing, ordering bloods, retrieving results, recording allergies, looking up X-rays and scans.
Most hospital systems have training resources — find them. Many have YouTube walkthroughs too.
Poor typing speed is one of the most underrated barriers to efficiency in both hospital and GP work. If you are slow at typing, start practising immediately. TypingClub.com is free and effective. "Mavis Beacon Teaches Typing" software (available on Amazon) is also excellent for structured improvement.
📱 Log Into FourteenFish and Explore ▾
Log into FourteenFish 3–4 times in the first two weeks — just to get familiar. Don't try to do log entries yet. Simply learn where to click. It takes time to get used to, and the last thing you want is to be struggling with the interface at the same time as trying to write a meaningful log entry.
🌍 Does Your English Need Improving? Plan Now ▾
This section is for those who qualified outside the UK and are still developing English fluency. Be honest with yourself — do you need to improve? If yes, now is the time to start. By ST3, you will have the SCA exam, where English fluency is critical. There won't be time then to start learning.
To improve rapidly, you need to use English outside work — not just at work. If 60% of your life is in your home language, you will improve slowly. Aim for immersion where possible:
- Watch a TV series entirely in English
- Listen to English audiobooks (doctor-written memoirs work brilliantly — see book list below)
- Watch your favourite movies again — this time in English
- Speak to your children at home in English if possible
- Attend a language class or find a language exchange partner (search MeetUp app or online for something local)
- Find a language teacher or native English-speaking friend for 1-to-1 help
- If you are in a study group — consider asking everyone to speak in English rather than your home language during sessions
Two methods that build fluency fastest:
- Speak opportunistically — try to speak to as many people in English as you can, every single day. Make notes on your difficulty areas and bring them to your teacher, trainer, or English-speaking friend.
- Read aloud to a friend — ask a friend or teacher to listen as you read a story book aloud, and have them gently correct you as you go. This builds pronunciation, rhythm, and vocabulary simultaneously.
Books for English learning and consultation skills together:
- This Is Going to Hurt — Adam Kay
- The Doctor Will See You Now — Amir Khan
- The Inner Consultation — Roger Neighbour (you learn consultation skills AND language — two for one)
- Complications or Better — Atul Gawande
- SeaSickness — Peter Tate
A community of GP trainees and trainers learning together. A great place to ask questions, share experiences, and feel less alone in your training journey. → Join the Bradford VTS Learning Circle
Months 1–3 — Build Your Foundations
Assessments start, log entries bed in, courses are booked, and you're deepening your practice.
📅 Book Your Courses Early — At Least 6 Weeks in Advance ▾
You are an employee with a job to do. Study leave must be co-ordinated with your department — they cannot simply release you at a day's notice. Book at least 6 weeks in advance.
Priority courses for early in training:
- Basic Life Support (BLS)
- Adult and Child Safeguarding
- Specialty-relevant knowledge update (e.g. contraception, ECGs, spirometry, COPD, diabetes)
- Consultation Skills training course
- Courses specifically targeting IMGs if relevant to you
📚 Start Reading a Consultation Skills Book ▾
You're in a hospital post — but you are training to be a GP with 10-minute consultations. Reading a consultation skills book now gives you a head start that you will thank yourself for later. Many trainees wait until ST3 and then wonder why their consultation style feels rushed and clumsy.
Hospital clerk-ins take 20–30 minutes. GP consultations are 10 minutes. These books will make you faster, more accurate, and better at explaining — useful right now on the wards, essential later.
If you enjoy narrative-style books:
- The Inner Consultation — Roger Neighbour. An old classic, still entirely relevant. Great storytelling narrative. [Paperback] [Kindle]
- Bedside Matters — Peter Tate and Francesca Frame (2020). Conversational, modern, excellent reviews. [Paperback] [Kindle]
If you prefer direct, structured books:
- The Doctor's Communication Handbook — Peter Tate. A classic. [Paperback] [Kindle]
- The Naked Consultation — Liz Moulton. A great all-rounder covering difficult situations. [Paperback] [Kindle]
It's one of the best — the only evidence-based communication skills book out there, and very practical. But it's heavy going for ST1s and ST2s. Best reserved for ST3. For now, pick any of the four books above — they are all excellent. If unsure, head to Amazon, read the reviews, and pick whichever one grabs your fancy. They are all pretty good.
This is the definitive accessible guide to evidence-based medicine and the statistics domain that catches many AKT candidates off-guard. Start it in ST2, not ST3. Statistics questions test understanding, not calculation — you need to know sensitivity, specificity, NNT, NNH, likelihood ratios, and confidence intervals. Greenhalgh explains all of them clearly and usably.
→ Bradford VTS Communication Skills Database — a large collection of further resources on consultation skills
📝 You Should Now Be Writing 1 Log Entry Per Week ▾
By month 2–3, you should be settling into a regular log entry rhythm. Target: 1 per week, 4 per month.
- 3 of those 4 must be on clinical encounters (recorded as Clinical Case Reviews)
- The 4th can be on anything — an HDR session, a teaching event, a personal reflection
A simple rhythm that works: Commit the last week of every month to your "non-clinical" log entry. All other weeks: clinical case reviews. This removes the weekly decision fatigue of "what do I write about?"
Your GP Trainer can tell you whether your entries demonstrate sufficient reflection and evidence of learning. Don't find this out for the first time at your ARCP. Ask for feedback on your first 2–3 entries — it will save a lot of pain later.
✅ Start Your WPBA — Do a Mini-CEX and a CBD ▾
You need 2 mini-CEXs and 2 CBDs by the midpoint of the year (i.e. per 6-monthly post). Don't leave them all to the end.
- Mini-CEX: A direct observation of a clinical encounter by your supervisor. You are assessed on communication, clinical assessment, clinical management, organisation, professionalism, and overall competency.
- CBD: A structured discussion of a case you have managed — not to test knowledge, but to explore your clinical reasoning and professional judgement.
The responsibility to arrange these rests with you, not your trainer. Ask your supervisor. Do it now.
→ Bradford VTS: Mini-CEX resources
→ Bradford VTS: CBD resources
🏥 Remember: You Are Still Training to Be a GP ▾
This is one of the most common traps. Trainees get absorbed in the specialty and temporarily forget that their goal is general practice. We are not asking you to care less about the specialty — we are asking you to filter your learning through a GP lens.
Practical examples of GP-focused filtering:
- O&G post? Learn to manage heavy menstrual bleeding — don't spend all your time in theatre learning surgical techniques
- Respiratory post? Learn the management of COPD and asthma — not how to perform bronchoscopy
- Paediatrics post? Learn child development milestones, febrile illnesses, and safeguarding — things you will see constantly in GP
- Psychiatry post? Learn the management of depression, anxiety, and first-episode psychosis — the presentations that arrive in your GP surgery every day
📖 Read About How to Study Effectively ▾
Most of us were never explicitly taught how to study — and yet the research on effective learning is extensive and genuinely useful. Some of the methods we instinctively rely on (re-reading, highlighting) are among the least effective. Some that feel uncomfortable (spaced repetition, testing yourself) are the most effective.
ST1 is the ideal time to audit your study habits and make changes — before the pressure of exams in ST3 arrives.
🎤 Consider Running a Teaching Session at HDR ▾
Teaching is a Professional Capability — and it is far harder to do well than most people assume. If you are asked to do a teaching session (at HDR, at a departmental meeting), prepare properly. Learn some basic teaching theory before you do it — not just to be good at it, but to understand why some teachers are more effective than others.
Last 3 Months — Consolidate & Complete
The final stretch. Time to close the loop on assessments, QI, ES meetings, and PDPs.
🔍 Review Your ePortfolio — Honestly ▾
Look at your ePortfolio with fresh eyes. Ask yourself:
- Are my log entries showing genuine reflection and learning — or are they descriptive accounts of what happened?
- Have I linked log entries to Clinical Experience Groups appropriately?
- Is there clear evidence for the 13 Professional Capabilities?
- Am I keeping to 4 log entries per month?
If things are going badly — discuss this with your GP Trainer now, not at the ARCP panel.
✅ Complete Remaining Mini-CEX and CBD ▾
By the end of the post, you need a minimum of 2 × mini-CEX and 2 × CBD from this placement. Aim for more — demonstrating more than the minimum is evidence of a committed, autonomous learner.
This is one of the most visible signs of poor self-management in a trainee's portfolio. Your trainer will notice. The ARCP panel will notice. Spread assessments throughout the placement — that is the point of doing them.
🔬 Start (or Complete) Your QI Project ▾
A Quality Improvement (QI) project is a mandatory requirement before the end of ST1. It is non-negotiable.
Keep it simple. Pick an area you find genuinely interesting — you will enjoy it more and produce better work. Discuss with your trainer early and choose something achievable.
Leave it to ST3 and it becomes a source of serious stress at the worst possible time. ST1 is the window — use it.
📋 Review and Update Your PDP ▾
A Personal Development Plan (PDP) should contain 3–5 SMART goals for each post:
- Specific — clearly defined goal
- Measurable — how will you know you've achieved it?
- Attainable — realistic given your workload
- Realistic — "attend a course" is realistic; "read 10 textbooks" is not
- Time-bound — with a clear deadline
Review how many PDP items you have achieved. If most are not done — this is a conversation to have with your trainer, not something to hide in the portfolio.
📊 Get Your ESR & CSR Done — Properly ▾
Your Educational Supervisor Review (ESR) and Clinical Supervisor Review (CSR) feed directly into ARCP panels. These panels determine whether you can progress to the next ST year. Take them seriously.
Three sections of your ES prep form — give each one proper time:
- "Finding the evidence for the Capability Self-Rating Scales"
- "Formulating action points for the capabilities"
- "PDPs" — review and update these
Expect an ES meeting to last 2–3 hours. Arrive prepared — your ES can see whether you have put effort in.
Also ask your Clinical Supervisor to complete a CSR — this is easy to overlook.
→ Bradford VTS: Educational Supervision pages
→ Bradford VTS: ARCP — what to expect
🎤 Continue Using Hospital Posts for SCA Preparation ▾
Every clinical encounter is an opportunity to practise the consultation skills you will need in the SCA. Pick one small area from your consultation skills book each week and practise it deliberately.
- Week 1: Focus only on opening — how you greet and establish rapport
- Week 2: Focus on exploring ICE (Ideas, Concerns, Expectations)
- Week 3: Focus on structuring explanations clearly
- Week 4: Focus on safety-netting
This deliberate practice in ST1 and ST2 means your ST3 GP trainer can polish your skills to a high level — rather than building from scratch.
WPBA at a Glance
The numbers you need to know — at a glance. Note: these are minimums. More is always better.
| Assessment Type | Where Done | Per 6-Month Hosp Post | Per Full ST Year | Notes |
|---|---|---|---|---|
| Mini-CEX | Hospital only | 2 minimum | 4 (if all hospital) | Direct observation of clinical encounter |
| CBD | Hospital or GP | 2 minimum | 4 per ST year | Structured case discussion exploring reasoning |
| COT | GP only | N/A in hosp | 2 (if 6m GP + 6m hosp) | Consultation observation — replaces mini-CEX in GP posts |
| Log Entries | Any post | ~4 per month | ~24–26 per year | 3 clinical (Clinical Case Reviews) + 1 other per month |
| MSF | Any post | 1 per post | Ongoing | Multi-source feedback from colleagues and patients |
| CSR | Any post | 1 per post | Per placement | Clinical Supervisor's Report — don't forget to ask for this! |
| QI Project | Any post | 1 in ST1 total | Mandatory before end ST1 | Start in ST1 — do not leave for ST3 |
| PDP | Any post | 3–5 items per post | Updated each rotation | SMART goals agreed with your trainer |
| CEPS | Best in hospital | As available | Complete during training | Clinical Examination & Procedural Skills — do them now, not in GP |
If your ST1 or ST2 is split between 6 months GP and 6 months hospital: you need 4 × CBDs + 2 × COTs + 2 × mini-CEXs by year end. If the entire year is hospital posts: 4 × CBDs + 4 × mini-CEXs.
🔬 CEPS — Clinical Examination & Procedural Skills
Hospital posts are the ideal setting for CEPS. You see patients daily with genuine clinical findings. In a GP post, finding enough patients for observed examinations is significantly harder. Use your hospital time strategically.
🫁 7 System Categories (Range Required Across Training)
- Respiratory system
- Ear, Nose and Throat
- Abdominal system
- Cardiovascular system
- Musculoskeletal system
- Neurological examination
- Child 1–5 years
You must demonstrate a range across training — aim for at least 2–3 CEPs per post. Do not leave any category entirely to the final GP placement.
🔐 5 GMC-Mandated Intimate Examinations
These must be performed competently and observed. They cannot be signed off retrospectively from memory.
- Breast examination
- Rectal examination
- Prostate examination
- Male genital examination
- Female genital examination (bimanual + speculum)
Intimate CEPs are best achieved in O&G or relevant surgical/medical posts with specialist nurse assessors. Arrange these early in the post — do not leave them to ST3 where the opportunity may simply not exist.
| Hospital Post | Best CEPs to Target | Why |
|---|---|---|
| Respiratory | Respiratory system CEP | Daily access to genuine respiratory signs |
| Paediatrics | Child 1–5 years CEP | Dedicated paediatric assessors and patient mix |
| O&G | Female genital (bimanual + speculum), Breast | Specialist assessors; dedicated examination opportunities |
| Cardiology / Medicine | Cardiovascular, Abdominal | High patient volume with genuine examination findings |
| Surgical / Urology | Rectal, Prostate, Male genital | Procedural context with trained assessors |
| Neurology / Medicine | Neurological examination | Access to genuine neurological signs |
| ENT / Surgical | ENT examination | Specialist equipment and assessors |
🏥 Ward Survival: Prioritisation, Escalation & Documentation
These are the skills that protect patients and protect you. They are also the skills that IMGs, early ST1s, and trainees coming from different healthcare cultures most often need explicit teaching on.
⚡ The Sick-First Rule — Clinical Prioritisation
When you have 10 jobs and 3 bleeps, use this order every time without exception:
Airway / Breathing / Circulation problems
Any patient with ABC compromise — see immediately.
Deteriorating observations / NEWS concerns
Rising NEWS score or nursing concern about a patient's baseline.
Chest pain / collapse / sepsis / reduced consciousness
Any acute presentation that could deteriorate rapidly.
Urgent jobs
Results to chase, urgent prescriptions, nursing requests that imply change from baseline.
Routine work and admin
Only after the above are handled.
Insider tip: A nursing concern is almost always clinically relevant. When a nurse says "I'm not happy with this patient," stop what you're doing and go and see. They see these patients all day. You see them once.
🗣️ Safe Escalation Phrases — Say These Out Loud
Early escalation is a sign of clinical intelligence, not weakness. These phrases help you escalate confidently and clearly.
Critical teaching point: Escalating early does not make you look weak. Delaying escalation out of fear of looking incompetent is what makes you unsafe. Your senior would rather be interrupted 10 times unnecessarily than miss the one time it mattered.
📋 Clinical Documentation — What to Record Every Time
📝 The Five Things to Record
Based on GMC Good Medical Practice — clear, contemporaneous, accurate records.
- What you found — examination findings, observations, relevant history
- What you thought — your working diagnosis and reasoning
- What you did — investigations ordered, treatments given, referrals made
- What you told the patient (or team) — information shared, consent, plan explained
- What the contingency plan was — if X, do Y; review timing; escalation triggers
"Patient stable" as a note is clinically and medico-legally unsafe. It tells the next doctor nothing about what you actually found, thought, or decided. Write your reasoning.
🤝 The Handover Formula
Poor handover is one of the commonest causes of preventable patient harm in hospitals. Use this structure every time:
- Who — name, age, location, relevant background
- What — the current problem
- What changed — what is different from baseline
- What you're worried about — your clinical concern, even if unconfirmed
- What needs doing — specific action required
- By when — urgency and timeframe
This structure maps directly onto SBAR (Situation, Background, Assessment, Recommendation) which many hospitals use formally. Learning it now means it becomes automatic.
A six-step mental framework for reviewing any hospital patient with a GP mindset:
Prioritise urgency — sick or stable?
Sick or stable? — use obs + ABCDE mindset
Assess focused red flags — name them
Form working diagnosis and plan
Escalate / explain / document
A simple safety-netting framework — works in hospital explanations and GP consultations alike:
Alarm features specifically named
Follow-up timing made explicit
Escalation route given ("go to A&E / call 999 / call us")
Return advised if worsening or worried
🚨 Red Flags to Recognise in Every Hospital Post
These are the presentations that require immediate action — and which GPs must recognise when they present in primary care too.
- Chest pain with concerning features (ACS / PE / dissection)
- Acute breathlessness or unexpected hypoxia
- Sepsis features (fever / tachycardia / hypotension / confusion)
- New confusion or reduced consciousness
- Acute abdomen
- Stroke or TIA symptoms
- Suicidal intent / acute psychosis / severe safeguarding concern
- AKI with dehydration, sepsis, or nephrotoxic drugs
- GI bleed
- Postpartum or pregnancy-related acute deterioration
💬 Choosing Good CBD Cases — What Makes a Strong One
A CBD is not about getting the right answer — it is about demonstrating professional judgement under uncertainty. Choose cases that have these features:
- Genuine diagnostic uncertainty — not a straightforward textbook presentation
- Risk-benefit weighing — where you had to balance competing considerations
- Appropriate senior advice sought — this demonstrates professional behaviour, not weakness
- An ethical dimension — consent, capacity, confidentiality, or conflicting interests
- Patient safety as a consideration — recognising or responding to a safety risk
After each mini-CEX, write a Clinical Case Review log entry on the same case. It takes 15 minutes and gives you both a WPBA and a portfolio entry from a single clinical encounter.
📅 Critical Timing Rules for WPBA and Supervision
- First mini-CEX and CBD: Month 2 — not Month 5. Do not wait until the post feels comfortable. The formative value of early assessments is real.
- Use different observers for each mini-CEX — ideally different consultants or registrars. This broadens your evidence base and avoids over-reliance on one assessor's lens.
- Mini-CEX assessment: no more than 15 minutes — including feedback. Keep this tight and purposeful.
- Request your CSR in Month 5 — not the final week. Give your Clinical Supervisor time to write a meaningful report. A rushed last-week CSR rarely reflects the full breadth of your performance.
Sick leave reminder: Both too much and too little sick leave can signal self-management problems to supervisors. Presenteeism — attending when genuinely unwell — is clinically unsafe and will raise concerns. If you are unwell, stay away. If you are struggling, seek support early.
Common Pitfalls & Trainee Traps
These are the patterns that come up again and again. Every one of these is a genuine mistake that has been made by real trainees. None of them need happen to you.
It is visible, it looks unprofessional, and your trainer will not be impressed. The assessments are meant to be spread throughout the post — that is the entire educational point of them. Set calendar reminders at the start of every placement.
"I saw a patient with chest pain. I took a history and examined them. They were discharged." This tells the ARCP panel nothing about your professional development. The question is: what did you learn and what will you do differently?
Trainees absorbed in the specialty often develop excellent secondary care skills but make no progress on the things that matter for GP training. Keep your GP lens on at all times. Ask: "How will this help me in 10-minute consultations?"
The ward sister, the HCA, the ward clerk — these are the people who often know the most about how the department actually works. Trainees who ignore non-medical staff miss out on crucial practical knowledge and damage a relationship that would have been enormously helpful.
Your ePortfolio tells the story of your training. If you only engage with it at crisis points, that story is thin, rushed, and unconvincing. Regular entries written thoughtfully throughout the year look entirely different to a last-minute dump.
Some trainees skip the scheme induction because "the hospital won't release me." This is not acceptable — and it is avoidable if you book it early enough. Contact your GP scheme administrator on day one of your post.
Every consultation in hospital is an opportunity to practise. Trainees who don't start developing their consultation model until ST3 GP often struggle — their trainer then has to teach fundamentals instead of polishing existing skills. Don't make this mistake.
A QI project needs time. It is harder to do in ST2 with demanding hospital shifts. It is nearly impossible in ST3 alongside the SCA and AKT. ST1 is the window. Use it.
For IMGs whose spoken English needs development — two years feels like a lot of time until it isn't. The SCA will test your ability to communicate naturally and fluently with patients. Start building that fluency in real English contexts now, not in the year of the exam.
You can tag up to three capabilities per entry — and you should. Most clinical encounters evidence multiple capabilities simultaneously (e.g. a complex discharge involves Clinical Management, Communication and Consulting, and Organisation, Management and Leadership). Under-tagging means under-evidencing. Review every entry before saving and ask: what else does this demonstrate?
CEG tagging needs thought, not a default click. A paediatric A&E case → "Infants, children and young people." A gynaecology case → "Women's health." A mental health review on the ward → "Mental health." Consistently tagging the wrong CEG means your portfolio will show gaps in clinical breadth that an ARCP panel will notice — even if you actually covered those areas.
Insider Pearls & Real-World Wisdom
The things that only become obvious after trainees have been through a placement. Here they are, up front, for you to read in week one.
- The ward sister usually knows more about departmental protocols than most junior doctors. Ask her. She will not judge you for asking.
- Consultations in hospital do not have to be ward-round style data dumps. Patients remember the doctor who took two extra minutes to explain what was happening.
- Start your ePortfolio early and write a little often. A well-maintained ePortfolio feels effortless; a rushed one feels dreadful and shows.
- The ARCP panel does not know you as a person. Your ePortfolio is the only version of you they see. Make it count.
- You get one chance to make an impression in the first week of a new post. Arrive on time, say hello to everyone, and ask questions. That's it.
- They start each post with a clear PDP — agreed with their trainer — and they actually look at it again mid-placement.
- They do WPBAs spread across the whole placement, not in a final-week panic. This alone signals an excellent trainee.
- They see every clinical encounter as an opportunity to practise something specific — not just to "see the patient and move on."
- They keep a brief clinical diary or "case of the week" note. When it comes to writing log entries, they have a rich source of material to draw on.
- They build genuine relationships with their supervisor — not transactional ones. The quality of their training shows it.
- They don't wait for the perfect case before writing a log entry. Every case — even a routine chest infection — becomes a powerful entry if you reflect deeply on what it revealed about your clinical reasoning, communication, or professional development.
- They are visible learners. The best CSRs come from trainees who regularly discuss their cases with their consultant, ask for feedback, and are seen to be actively developing. A consultant who never sees you reflect will never know you do.
Each time you see a patient in hospital, ask yourself: "How would this presentation arrive in general practice? What would I do with 10 minutes? What primary care management should this patient have received before they got here?" This habit transforms a service job into active GP training.
Your GP Trainer will not chase you for WPBAs, log entries, or PDPs. This is intentional. GP training is designed to develop autonomous learners — doctors who take responsibility for their own development. If you are waiting to be reminded, you are training yourself into dependence. The trainee who asks is the trainee who grows.
On-calls are the best time in a hospital post to capture Mini-CEX and CBD opportunities. Clerking a new patient, reviewing a deteriorating patient, or discussing a management decision with a senior are all ideal triggers for WPBA. Ask your registrar or consultant at the end of a case: "Would you be happy to do a quick Mini-CEX on that?" The case is fresh, the assessor is there — it takes 10 minutes. Do not wait until next week.
Do not let your entire hospital post become ward-only service work. Deanery quality standards describe outpatient or comparable exposure as reasonable and important. One relevant clinic or MDT per fortnight is a realistic target in most specialties. Outpatient exposure gives you the GP-relevant decision-making (diagnose → plan → refer back → safety-net) that ward work alone often does not.
As of 2025–26, assessors need a free FourteenFish account before they can sign off any WPBA. This means your consultant or registrar must register before they can complete your mini-CEX or CBD. Tell your supervisor at the very start of the rotation — not the week you need the assessment signed. Hospital seniors are frequently unaware of this requirement.
Create a shared folder at the start of every post and populate it with: paediatric traffic light criteria, FRAX score guide, BNF emergency summaries, local referral pathways, and common treatment regimens for your specialty. This is a practical clinical resource AND evidence of self-directed learning — reference it in your PDP.
At the start of every rotation, say to your consultant or registrar: "I'm a GP trainee — I need to complete 2 mini-CEXs and 2 CBDs this post. Could I flag when I'd like one done?" This prevents last-minute scrambling, ensures they have a FourteenFish account in time, and immediately signals that you are an organised, autonomous trainee.
Common trainee complaint: "The senior made all the decisions — I didn't do anything." The fix: write what you were going to do, then compare it with what the senior actually did — and why. This demonstrates clinical reasoning, self-awareness, and learning from experience — exactly what ARCP panels want to see. The most powerful log entries are often written after cases where you observed, not acted.
"It is not enough to be good. You must leave evidence that you were good."
The ARCP panel judges you solely on your ePortfolio. An ePortfolio with 4 entries per month, spread evenly across capabilities and CEGs, written with genuine insight, is worth far more than 20 entries written in the last two weeks of a post. The quality of your evidence is the only version of you they see.
The "Management" pillar includes managing yourself. Happy, grounded doctors make better decisions and fewer errors. Variable shift patterns in hospital posts are one of the most cited causes of burnout in GP trainees. Build in deliberately:
- Protected meal breaks — away from a desk, not at the workstation
- A consistent handover time — and a clear point at which the working day ends
- Regular exercise and scheduled social activities — this is not self-indulgent, it is clinically necessary
If your wellbeing is suffering — speak to your GP Trainer or Educational Supervisor. If things are serious, speak to your own GP or Occupational Health. There is no virtue in suffering quietly, and there is no shame in seeking support. The profession needs you well.
Using Hospital Posts to Prepare for the SCA
The Simulated Consultation Assessment (SCA) in ST3 is the exam that catches trainees most off-guard. It tests communication, consultation structure, and human connection under pressure. Every hospital consultation is an opportunity to start building those skills now.
🎯 What the SCA Actually Tests
The SCA tests three domains: Data-gathering and diagnosis, Clinical management, and Relationship and communication. The third domain is where trainees most commonly lose marks — and it is entirely trainable.
Hospital consultations test all three domains too — if you make them. A ward admission is data-gathering. A medication discussion is management. Explaining a diagnosis to a frightened patient is relationship and communication.
📚 The Consultation Model to Learn Now
The core consultation model you will be tested on combines:
- History and examination (clinical gathering)
- ICE — Ideas, Concerns, Expectations
- PSO — Patient's Social and Occupational context
- Shared decision-making
- Safety-netting
Reading one consultation skills book now means your GP trainer can build on foundations in ST3, not lay them.
🗣️ Consultation Phrases to Start Practising Now
These are the natural, human phrases that work in the SCA — and in every real consultation. They should not feel scripted. Practise them until they become your voice.
Experienced examiners report that the single most common reason trainees fail the SCA is not clinical knowledge — it is failure to genuinely explore the patient's Ideas, Concerns, and Expectations. Candidates who ask "What were you worried it might be?" and then actually listen and respond to the answer score dramatically better. Start practising this in every hospital consultation now.
⏱ The 12-Minute SCA Consultation Timeline
Use this as your mental template for every consultation — in the SCA and in everyday hospital practice right now. Trainees who fail typically spend 9 minutes on history and 3 on management. That ratio is detectable — and costly.
| Time | Focus | Why it matters |
|---|---|---|
| 0–1 min | Open, set agenda, establish main concern | Listen without interrupting for at least 60 seconds — trainees who interrupt within 30 seconds miss the patient's real agenda |
| 1–6 min | Focused data gathering (history, ICE, PSO) | Ask questions that matter — do not ask everything. Non-verbal cues (eye avoidance, tense body language) often signal unexpressed concerns |
| 6–7 min | Internal synthesis — working diagnosis / differential | If you reach minute 7 still gathering data, you are running behind — signpost the shift: "That's really helpful. Let me now explain what I think is going on." |
| 7–10 min | Explain, negotiate management plan, shared decisions | Say your reasoning out loud. "The reassuring features are..." "The reason I'm checking X is..." Negotiation beats prescription. |
| 10–12 min | Safety-net with specific triggers, follow-up, close | SAFER: Suspected diagnosis explained, Alarm features named, Follow-up timed, Escalation route clear, Return advised if worried |
This is a key examiner expectation that many trainees miss. Empathy, signposting, and checking understanding should be woven into every part of the consultation — not saved up for a dedicated block. Signpost every transition: "I'd like to ask a few focused questions first, then explain what I'm thinking — is that OK?" Name what you're doing. The examiner is watching for this throughout.
🏋️ Practical SCA Drills for Hospital Posts
Hospital posts give you 20–30 minutes per patient. Use that time to deliberately develop consultation skills — not just clinical clerking skills.
- After each clerk-in, self-check three things: Did I explore ICE? Did I explain the diagnosis in plain language? Did I safety-net with specific triggers?
- Pick one micro-skill per week from your consultation book (e.g. open questions, summarising, signposting) and deliberately practise it in the next five consultations.
- Record one consultation per week on video where possible and review it. Neighbour's Inner Consultation recommends this explicitly. You will notice things you simply cannot notice in real time.
- Attend to non-verbal cues — eye contact avoidance, tense body language, and fidgeting often signal unexpressed concerns that ICE alone will not surface. Name what you observe: "You seem a little tense — is there something else on your mind?"
🎯 Additional SCA High-Yield Pearls
⏱ The 6–7 Minute Rule
The RCGP SCA toolkit is explicit: good candidates usually complete data gathering by 6–7 minutes of a consultation, leaving sufficient time to build and discuss the management plan with the patient.
Candidates who over-run on history-taking run out of time to demonstrate shared decision-making and safety-netting — the domains where many marks are lost.
Practise in hospital: Time your clerk-ins. Aim to have your working diagnosis and key ICE explored within 7 minutes. Then consciously shift into explanation and planning mode. This habit becomes automatic in GP.
🩺 Behave Like a GP — Not a Frightened SHO
A repeated theme in SCA feedback: candidates over-investigate, refer everything, and behave as though they are in a hospital emergency rather than a GP surgery. SCA rewards safe, proportionate general practice.
- Ask yourself: "Can I manage this safely in GP with appropriate review?"
- Unnecessary referrals can lose marks — they can signal poor clinical confidence
- Uncertainty must be managed proportionately, not by blanket investigation
- A clear, reasoned plan with good safety-netting beats defensive medicine every time
- Don't interrupt within 30 seconds — trainees who cut across the patient's opening statement regularly miss the real agenda. Give them a full minute before narrowing.
- Negotiate, don't prescribe — "I'll prescribe X" is a tell. "What are your thoughts on trying X?" is a pass. The difference is shared decision-making vs dispensing.
- Always close explicitly — summarise the plan, confirm the patient understood it, and safety-net with specific triggers. Forgetting to close is a mark-losing omission.
🔄 The Micro-Summary Technique
The RCGP toolkit is explicit that repetition damages rapport, wastes time, and signals poor listening. The fix is micro-summaries:
Micro-summaries confirm understanding, signal good listening, and move the consultation forward efficiently. Practise them in every hospital clerk-in.
🌍 Useful Phrases if English is Your Second Language
Confident, clear clinical language under pressure is a learnable skill. Practise these short, natural phrases until they become automatic:
Analysis of uncertainty and decisions — what was hard?
Evidence of learning and change — what will you do differently?
🗣 Consultation Phrases for Hospital Posts
Hospital consultations are not just clinical transactions — they are communication opportunities. Every ward clerk-in, every bedside conversation, every discharge explanation is a chance to practise phrases you will need in the SCA and in GP practice. Memorise the principle. Then adapt to your own voice.
Don't try to memorise everything. Pick one skill area each week and use it deliberately in every relevant encounter — ward clerk-ins, discharge conversations, breaking news, explaining diagnoses. Repetition across dozens of real patients is worth more than reading a phrase list once.
🚪 Opening & Agenda-Setting
Works for ward clerk-ins, outpatient consultations, and any first encounter
💭 Exploring Ideas (ICE — Thoughts)
Genuinely listen to the answer — that's where the gold is
Avoid: "Do you have any ideas?" — too closed. Also avoid using the word "ideas" itself — it sounds clinical and scripted to patients.
😰 Exploring Concerns (ICE — Worries)
This is often the most important question in any consultation
🙋 Exploring Expectations (ICE — Hopes)
Understanding what the patient wants often resolves the whole consultation
🤝 Empathy — Interpretive, Not Generic
Name the specific emotion and link it to their situation — generic empathy rings hollow
Avoid: "I understand how you feel" — you cannot understand their specific experience, and patients often sense the hollowness of it.
➡️ Signposting to Management
Signals a gear-change so patients follow the structure of the conversation
💬 Explaining & Reasoning
Lead with evidence, arrive at diagnosis — the patient anticipates rather than argues
🤔 Handling Uncertainty
Honesty about uncertainty builds more trust than false confidence
🤝 Shared Decision-Making
Involvement is not a formality — patients who help choose their plan are more likely to follow it
🛡 Safety-Netting — Specific & Actionable
Word order rule: end on a positive expectation — the last thing said is best remembered
Avoid: "Come back if worried" alone — too vague to constitute meaningful safety-netting, and it won't score marks in the SCA either.
✅ Checking Understanding
Ask them to recall — not just confirm. "Does that make sense?" gets a reflexive yes. These get real answers.
🏥 Hospital-Specific Situations
Phrases for moments that come up most in inpatient and ward settings
Explaining why they're being kept in:
Explaining a test or investigation:
Explaining discharge and what happens next:
➕ Additional Phrases Worth Adding to Your Repertoire
Opening variants
Concerns — deeper follow-up
Richer shared decision-making
Closing — confirm plan retained
📋 Adaptable Consultation Templates
These are structural frameworks — not scripts. The words should be yours. Practise the sequence in hospital until it becomes instinctive.
🔬 Template 1 — Undifferentiated Presentation
Open
"Tell me what's been happening." — Listen without interrupting for at least 60 seconds.
Data gathering
Focused questions based on red flags and differentials — not everything.
ICE
"What do you think is causing this?" / "Anything worrying you?" / "What were you hoping I could help with today?"
Interpretive empathy
Name what you heard: "It sounds like this has really been affecting your day-to-day life."
Plan
"Here's what I think is going on, and what I'd suggest..." → Negotiate, don't prescribe.
Safety-net
Specific triggers, specific timeframe, specific action. Not "come back if worried."
Close
"Any questions?" → Summarise plan in 1–2 sentences. Check they can tell you back the plan.
💔 Template 2 — Breaking Bad or Difficult News
Hospital posts give you regular opportunities to observe and practise this. Start now — don't wait for GP land.
Check prior knowledge
"Before I share what I've found, can I ask what you already know — or what you were expecting?"
Warning shot
"I'm afraid the results aren't quite what we'd hoped."
Give the news slowly
Plain language. Short sentences. Then pause — do not rush past it.
Silence
Allow the patient to react. Resist filling the silence immediately. This is one of the most important clinical skills.
Empathy
"I can see this is a lot to take in."
ICE revisited
"What's going through your mind right now?"
Next steps + safety-net
Explain what happens next clearly. Don't overwhelm. Say who to call, when they'll hear from you next.
Every phrase above follows one underlying rule: treat the patient as a partner, not a recipient. You are not delivering information to them — you are working through it with them. This shift in stance, practised consistently in hospital, will transform your GP consultations and your SCA performance. It cannot be faked; it has to become how you actually think.
Trainer & TPD Pearls
Guidance for GP trainers, educational supervisors, and TPDs supporting trainees in hospital posts.
🎓 Common Trainee Blind Spots in Hospital Posts
- Not applying a GP lens to hospital work — focusing only on the specialty
- Writing descriptive log entries with minimal reflection
- Bunching WPBAs at end of placement
- Not building relationships with non-medical staff
- Not flagging English fluency needs early enough
- Forgetting the QI project until it becomes urgent
💡 Tutorial Topics for Hospital Placements
- "What are you learning from this placement that a GP actually needs?" — filters GP-relevant learning
- Log entry review — move from descriptive to reflective writing
- "Show me your PDP" — check it is SMART and progressing
- Breaking bad news role-play — essential in hospital
- Discussing a case through the CBD framework — teaches professional judgement
- "How are you finding the workload?" — wellbeing check-in
At the Placement Planning Meeting (start of each post), explore what the trainee wants to develop in each of the 4 pillars. A trainee with specific, self-generated goals for each pillar is already demonstrating autonomous learning behaviour — one of the core aims of GP training.
Decision-Making at ST1/ST2 level: all patients should still be debriefed for safety. A trainee who stops seeking input too early is a clinical risk. Look for this in the CSR narrative and in supervisor discussions.
- "If you were a GP receiving a referral letter from this department, what would you want it to say?"
- "What did this specialty teach you about how GPs should manage this condition before referring?"
- "Tell me about a moment this post where you were unsure what to do. What did you learn from it?"
- "How would your Mini-CEX cases look different if you did them again now vs. at the start of the post?"
- "What is the most important thing this placement taught you about yourself as a doctor?"
Frequently Asked Questions
The questions that come up again and again — answered directly.
🔢 How many mini-CEXs and CBDs do I need per hospital post?
Per 6-month hospital post: a minimum of 2 × mini-CEXs and 2 × CBDs. By the end of a full ST year in hospital: 4 × mini-CEXs and 4 × CBDs. If your year is split between GP and hospital, the numbers adjust proportionally — see the WPBA table above.
🔄 Can I do a CBD in a hospital post?
Yes. CBDs can be done in both hospital and GP posts. Hospital consultants can act as CBD assessors during hospital placements. Mini-CEXs, however, are done in hospital posts only (COTs replace them in GP posts).
❓ Do I need to do a QI project in every post?
No. You need to complete one QI project before the end of ST1. This is a mandatory training requirement. Start planning and discussing it with your trainer early in ST1 — it needs more time than most trainees expect.
📝 How many log entries do I need to write?
Target: 1 per week, 4 per month. Of those 4: 3 must be Clinical Case Reviews (about patient encounters), and 1 can be about any learning activity (HDR, tutorial, course, etc.). The key is consistency — regular, thoughtful entries throughout the year, not a batch written the week before ARCP.
🌍 I qualified overseas — what should I prioritise in my first hospital post?
Three priorities above all others:
- English fluency — if this needs work, start now. Immersion outside work (TV, books, social conversation in English) matters as much as work exposure. The SCA in ST3 will test you hard on this.
- UK NHS systems and culture — understand team-working, the non-hierarchical ward culture, and the ePortfolio requirements. These are genuinely different from many international systems.
- Consultation skills — start reading a consultation skills book and begin practising ICE in every patient encounter. Don't wait until ST3.
⚡ My trainer has not mentioned my ARCP or WPBAs. Should I wait for them to bring it up?
No. In GP training, the expectation is that you manage your own professional development. Your trainer will not remind you when assessments are due — this is by design. It is developing your autonomy as a learner. Ask your trainer to do a mini-CEX or CBD. Arrange it yourself. Don't wait.
💻 How often should I be logging into FourteenFish?
In the first two weeks: 3–4 times just to get familiar with the interface. After that: at least once or twice a week to add log entries or update progress. Many trainees find it helpful to set a fixed time — for example, every Sunday evening for 20 minutes. Consistency matters more than volume in any single sitting.
😬 I'm finding the workload really difficult. Is this normal?
Yes — but "normal" doesn't mean you shouldn't get support. Hospital posts in ST1 and ST2 can be genuinely demanding. If you are struggling with the clinical load, speak to your registrar or consultant. If you are struggling personally or emotionally, speak to your GP Trainer or Educational Supervisor. If things are serious, speak to your GP or Occupational Health. Looking after yourself is part of your training — not a distraction from it.
Key Bradford VTS Resources
Everything you need — one click away.
🗺 What Other UK VTS Schemes Emphasise
Different schemes approach hospital posts slightly differently. Knowing what other training programmes prioritise can sharpen your own approach — and these resources are all freely accessible wherever you train.
🏫 Coventry & Warwickshire VTS
Runs separate teaching sessions titled "Preparing for Training" (ST1), "Preparing for Assessment" (ST2), and "Preparing for Practice" (ST3) — a useful framework for self-pacing your own learning journey. Also provides specialty-specific hospital guides explaining what each rotation offers for GP training.
→ Useful model: think of each ST year as having a distinct learning focus beyond just "doing the job."
🏫 Mid Sussex & Brighton VTS
Mandates a minimum of 2 VTS half-day release (HDR) sessions per 4-month hospital post, booked with at least 6 weeks' notice. Trainees in hospital posts may attend either Brighton or Mid Sussex HDR sessions for flexibility.
→ Key takeaway: HDR attendance from hospital posts is expected — book it early, it is not optional.
🏫 Thames Valley
Offers a dedicated Consultation Skills Day for ST1 trainees — an introduction to GP consulting with structured feedback. FourteenFish has been adopted formally across the region. Also uses a 60% allocation model for secondary care and ST1/ST2 posts to enable slot-sharing.
→ Key takeaway: consultation skills training should begin in ST1, not ST3.
📖 GP Trainee's Survival Guide (Independent Resource)
This independent resource recommends aiming for 2 log entries per week (one clinical, one other) and emphasises strategic capability coverage — ensuring every capability area has at least 2 entries across a training year. Somerset VTS formally endorses this 2-per-week target for ST1/ST2.
→ thegptraineessurvivalguide.com — worth bookmarking.
Every scheme emphasises the same core principles: spread your assessments, keep your portfolio active throughout, use hospital time to build consultation skills, and treat GP training requirements as non-negotiable regardless of how busy the wards are. The details vary — the expectations do not.
Final Take-Home Points
You are a GP trainee in a hospital — not a hospital doctor who happens to be a GP trainee. Keep the GP lens on at all times.
The 4 pillars — Relationships, Decision-Making, Management, Professionalism — underpin everything. Know them. Use them. Develop all four.
Spread your WPBAs across the whole placement. Two at the start, two at the end. Not all in the final fortnight.
Your ePortfolio is the only version of you that the ARCP panel sees. Write it like it matters — because it does.
Hospital wards are not hierarchies. The doctor is one cog in a system that needs every cog. Get to know everyone. They will make your life better.
Start your consultation skills book now. Don't wait for GP land. Every hospital encounter is a chance to practise the ICE framework that will matter enormously in your SCA.
QI project in ST1. Mandatory. Non-negotiable. Do it now — not in ST3 when you'll have the SCA, the AKT, and a full ST3 GP placement competing for your time.
If your English needs work — start now. Two years is a long time, until it isn't. Immersion works; occasional work exposure doesn't.
No one will remind you to do your WPBAs, log entries, or PDPs. That is by design. Own your learning. Be the trainee who asks.
Happy doctors are better doctors. Look after yourself. That is not separate from your training — it is part of it.
Bradford VTS is a free educational resource created by Dr Ramesh Mehay and contributors worldwide.
Medical Disclaimer · Support the site · Contact Us
In Every Post (Universal Principles)
Placement Planning Meeting (PPM): Within 3 weeks of starting, meet your clinical supervisor. Bring a written PDP — this immediately signals motivation and usually results in better teaching.
Ask: “What would this patient look like in GP?” — After every ward round, consider: What brought them to the GP first? What were the early signs? How could it have been managed in primary care?
Relate every case to a RCGP Topic Guide — Most cases map to one of 22 clinical topic guides.
Document your clinical case reviews within 48 hours while the clinical detail is fresh.