Quality Improvement
Because "we've always done it this way" is not a quality improvement strategy.
Quality Improvement (QI) is one of those topics that sounds daunting until someone explains it properly — then it suddenly feels not just manageable, but genuinely exciting. This page demystifies QI, explains what trainees actually need to do for their RCGP portfolio, and gives you the practical tools to do it well.
📥 Downloads
Handouts, summaries, and teaching extras — ready when you are. Clinical governance resources, QI frameworks, and project guides all in one place.
path: UNDERSTANDING QUALITY & QUALITY IMPROVEMENT
- breakfast as a metaphor for quality.doc
- clinical governance - a closer look.doc
- clinical governance - quality and economics.ppt
- clinical governance scenarios (TEACHING RESOURCE).doc
- clinical governance.ppt
- engaging team members in behavioural change.pdf
- examining the quality of care.pdf
- improvement science.pdf
- improving safety - critical events and critical error.doc
- involving patients in quality improvement.pdf
- learning culture of your environment.pdf
- measuring and monitoring safety.pdf
- NSF leads.ppt
- probophilia - quality versus quantity - are we counting the wrong things.pdf
- quality - donabedian-maxwell-wright.pdf
- quality - the donabedian way (with slide notes).ppt
- quality improvement made simple.pdf
- quality improvement wheel.pdf
- quality is a lousy idea.ppt
- quality of care by avedis donabedian.pdf
path: IDEAS
path: PROJECTS IN GP
- ethical approval for your research or project.pdf
- plagiarism - the thin grey line.doc
- project work in gp training.ppt
- projects - a generic marking crib.doc
- projects - how to decide on a topic area.doc
- projects - what makes a good one.pdf
- quality improvement methodology.pdf
- sample size calculator.xls
🔗 Web Resources
A hand-picked mix of official guidance and real-world GP training resources. Because sometimes the best pearls are not hiding in the official documents.
Core Official Resources
Bradford VTS Resources
Writing & Academic Skills
Data & Prescribing Tools
💡 What is Quality Improvement?
The definition you'll actually remember — and why it matters to you.
The Core Definition
Quality Improvement (QI) is an evidence-based, systematic approach to making healthcare better. It helps primary care teams deliver and evaluate initiatives, embed new practices more effectively, and use their systems, talents, and expertise more intelligently — all with the goal of better patient outcomes.
In short: it is the habit of continuously moving from where you are now to a better place. Not a grand annual project. Not a tick-box exercise. A mindset and a method.
🤔 Why Quality Improvement? We're already overstretched!
Up until recently, quality improvement in General Practice has been hard work. Doing big projects and big clinical audits on top of QoF, LES's, DES's, Appraisal, GP Training and so on has made it feel overwhelming and quite frankly HARD WORK!!!
This is because for far too long, the NHS has been too concerned with Quality Assurance rather than Quality Improvement. Quality Assurance is proving to others that we're doing a good enough job — and that's why it feels horrible. We're proving to others that we are meeting criteria and there's not much in it for us. It's far too focused on meeting a set of standards defined by someone else rather than just trying to move to a better place than we currently are.
QI is more focused on this movement to a better place. It's about accepting that we're not always great, not beating ourselves up about it, but actually working towards somewhere better. And unlike Quality Assurance, it is a process that doesn't just happen every now and then — it happens in small incremental steps, continuously.
As a result, it feels far less overwhelming, far more achievable, far more likely to improve the quality of care we provide as time goes by, and ultimately far more satisfying.
Isn't that what you'd like to be a part of?
…it's probably because all you have ever known is the Quality Assurance model and all the bits and bobs that go with it that cause us all a headache. These Bradford VTS pages — alongside the RCGP's QI Ready Online Toolkit — are provided to help you understand the Knowledge, the Skills, and the Attitudes necessary for Quality Improvement. And when you have that under your belt, you will feel well-equipped to engage.
If we train GP trainees up for it during their training, it puts them in a positive position to want to continue to engage when they qualify. Well — we hope so!
Quality Assurance vs Quality Improvement
This is the key distinction — and it explains why traditional quality work has felt so unrewarding.
😩 Quality Assurance (QA)
- Proving to others you meet a minimum standard
- Defined by someone else's criteria
- Happens every now and then (e.g. CQC inspection)
- Focused on compliance, not improvement
- Feels threatening and burdensome
- Little personal gain — lots of admin pain
- Results in paralysis or box-ticking
😊 Quality Improvement (QI)
- Moving your own team to a genuinely better place
- Defined by what you think matters
- Continuous — happens in small steps, all the time
- Focused on getting better, not proving adequacy
- Energising and professionally satisfying
- Directly benefits your patients and your practice
- Results in incremental, sustainable change
If QI has always felt like a chore, it's probably because you've been doing QA — proving to assessors and organisations that you're "good enough." Real QI is personal: you spot something that could be better, you do something about it, and you see the improvement happen. That's what the RCGP actually wants to foster — a culture of continuous, personally-driven improvement.
🔬 Frameworks for Understanding Quality
The conceptual models behind quality in healthcare — useful for your QI write-up and for discussions with your supervisor.
The Donabedian Framework — Structure, Process, Outcome
Avedis Donabedian's framework is the backbone of quality measurement in healthcare. Every QI project can be mapped onto this model.
Structure
The resources and conditions needed to deliver care
- Staffing and skill mix
- Equipment and facilities
- IT systems and software
- Policies and protocols
- Physical environment
Process
What is actually done in delivering and receiving care
- Clinical decision-making
- Prescribing patterns
- Referral behaviour
- Monitoring and follow-up
- Communication with patients
Outcome
The effects of care on patients and populations
- Clinical outcomes (e.g. HbA1c)
- Patient satisfaction scores
- Hospital admissions avoided
- Mortality and morbidity
- Patient-reported outcomes
Maxwell's 6 Dimensions of Quality
Robert Maxwell (1984) described six dimensions that together define quality in healthcare. When reflecting on your QI project, try to identify which dimension(s) you are addressing.
🎯 Effectiveness
Does the care achieve the intended result? Is evidence applied to practice?
🚪 Accessibility
Can patients access care when and where they need it, without excessive barriers?
⚖️ Equity
Is care fair? Are similar needs met similarly regardless of background?
💷 Efficiency
Is care delivered without waste? Are resources used to their best effect?
😊 Acceptability
Does care meet patients' reasonable expectations? Is it delivered humanely?
🌍 Appropriateness
Is care relevant to the patient's actual needs? Does it match the context?
⚡ Quick Summary — If You Only Read One Thing
The key points in sixty seconds. Ideal if the tutorial starts in five minutes.
🔑 Essential Take-Aways
- QI = moving towards a better place, continuously
- QA = proving to others you're good enough (feels rubbish)
- Trainees need 1 QIP + 2 QIAs by end of ST3
- QIP must be in a GP post (ST1 or ST2 preferred)
- QIA is smaller, quicker — focused on self OR practice
- PDSA = Plan, Do, Study, Act — the engine of QI
- Donabedian: Structure → Process → Outcome
- Evidence your QIP on FourteenFish ePortfolio
- Don't leave your QIP until ST3 — do it in ST1
- QI Ready toolkit (RCGP) is your best free resource
- Good QI needs a learning culture + patient involvement
- Measure before and after — no measurement = no QI
📋 RCGP Requirements — What You Must Do
The mandatory requirements, clearly laid out. No more confusion about what's expected by the time you reach your ARCP.
Requirements can be updated. Always verify with the RCGP WPBA page and check your deanery's local requirements. The table below reflects current guidance but your trainer and ES will confirm what applies to you.
| Training Year | Requirement | Key Points |
|---|---|---|
| ST1 | 1 × QIA per year + ideally 1 × QIP (if in GP post) |
The QIP is best done in ST1 — there's more time and space. Don't wait until ST3. The QIP must be completed during a primary care placement. |
| ST2 | 1 × QIA per year + 1 × QIP (if QIP not done in ST1) |
If you haven't done a QIP in ST1, do it now during your GP post. QIP done in ST1/ST2 counts as that year's QIA as well. |
| ST3 | 1 × QIA per year Leadership Activity (separate requirement) |
Focus on Leadership Project in ST3 — this is a separate RCGP requirement. QIA still required. QIP is ideally already complete. |
| By end of ST3 | Minimum total: 1 QIP + 2 QIAs | The QIP should be evidenced in the specific QIP section on FourteenFish ePortfolio. QIAs go in the Learning Log as reflective entries. |
- QIP: Use the dedicated QIP section on your FourteenFish ePortfolio (separate from the Learning Log)
- QIA: Evidenced as a Learning Log entry — your reflection must include what data you looked at, what you found, what action you took, and what changed
- Your supervisor assesses the QIP and provides graded feedback (below expectation / meeting expectation / above expectation)
- The assessment is formative — it is not a pass/fail, but it must be completed to satisfy ARCP criteria
⚖️ QIA vs QIP — What's the Difference?
This is the question every trainee asks. Here's the clearest possible answer.
According to RCGP rules, trainees have to show QIA every year. In the ST1 or ST2 year (when in a GP post) they have to do a Quality Improvement Project, and in ST3 they have to do a Leadership project. One would think that nearly all clinically orientated projects would automatically be demonstrations of Quality Improvement Activity — and indeed they are. So what is the difference, and why does the college want you to do QIA every year on top of a project? Well, this is what I think…
Quality Improvement Activity
- Smaller scale — hours to a day or two
- Quick, light, and focused
- Can focus on you as an individual OR on the practice
- Requires action — not just reflection
- No formal assessment form (goes in Learning Log)
- Required every training year
- Can be a mini-PDSA, a notes review, a prescribing review
- Must be systematic and involve a personal connection to your work
Quality Improvement Project
- Larger scale — weeks to months
- Meaty — involves data collection, change, re-measurement
- Always focused on practice/organisation improvement
- Must be in a primary care setting
- Uses a specific QIP template (RCGP provided)
- Formally assessed by your Educational Supervisor
- Minimum one complete by end of training
- Requires baseline data, intervention, and re-measurement
QIA things are easier to do. The college is trying to promote a culture where GPs in the UK are engaged with continuous and progressive development rather than just resting on our laurels and assuming we are okay. In the past, people got bogged down with projects — so the good thing about QIA is that they don't exhaust you. They are quick and light and pretty easy to do. But most importantly — they change you.
Quick Examples of QIA vs QIP
QIA Examples (quick)
QIP Examples (substantial)
🎯 QI Activity Types — What Can You Do?
Quality Improvement Activity comes in many forms. Each links to its own Bradford VTS page with more detail.
Clinical Audit
Compare practice against standards. Identify gaps. Close them. Re-audit.
📖Case Study
Detailed analysis of a single case or event for educational purposes.
💬Discussion Paper
A written exploration of a clinical or professional topic, drawing on evidence.
📚Literature Review
Summarise and appraise existing evidence on a GP-relevant topic.
🏥New Service Implementation
Designing, piloting, and evaluating a new clinical or administrative service.
📋Notes Review
Systematic review of consultation records to assess care quality.
🔄PDSA Cycles
Plan, Do, Study, Act — the engine of incremental improvement.
💊Prescribing Analysis
Review prescribing patterns and compare to guidelines and peers.
📊Questionnaires
Structured patient or staff feedback to identify areas for improvement.
📤Referrals Review
Review the appropriateness and quality of your outpatient referrals.
🧪Research Study
A formal research question, methodology, data collection, and analysis.
⚡Significant Events (SEA / LEA)
Structured reflection on a significant clinical or professional event.
Learning Event Analysis (LEA) and Significant Event Analysis (SEA) are separate mandatory requirements and do not count towards your annual QIA. You still need at least one QIA per year in addition to any LEA/SEA you complete.
❓ The 3 Fundamental Questions of QI
These three questions underpin every QI methodology. Whether you're doing a PDSA, an audit, or a QIP, you're always asking these three things.
What are we trying to achieve?
Understand the problem clearly. Define your aims and objectives. Be specific.
How will we know a change is an improvement?
Measure before and after. Decide what success looks like before you start.
What changes can we make that will result in improvement?
Look at what others have done. Form a hypothesis. Test it small, then scale.
There are tools that will help you define your question, aims, and objectives clearly — before you start collecting any data.
There are tools to help you measure processes and outcomes — so you can tell whether what you're doing is actually making a difference.
Then there are tools to help you evaluate your findings, present your data clearly, and help implement actions so that change actually sticks.
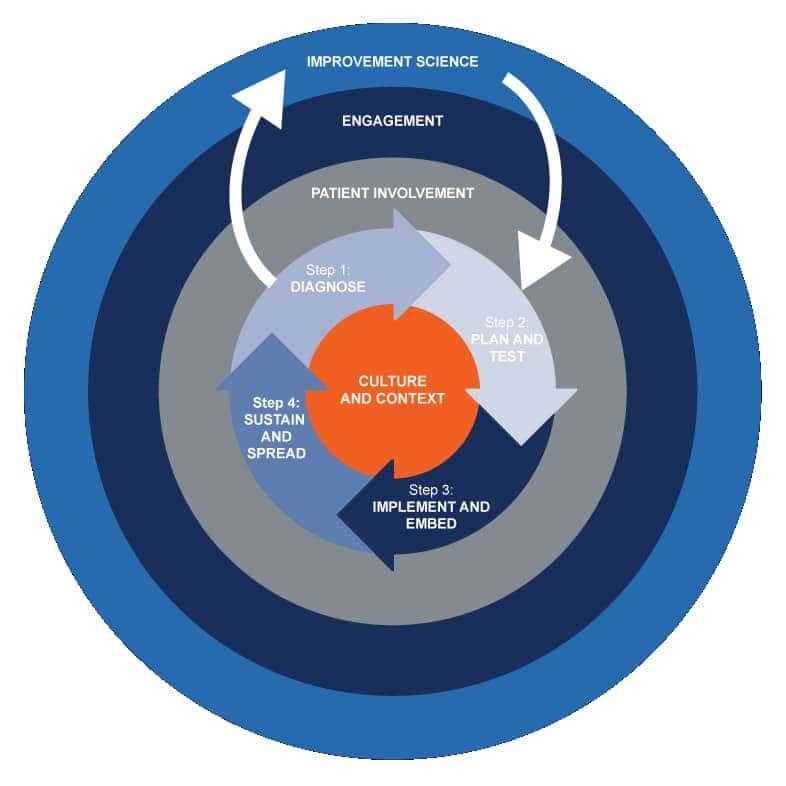
☸️ The QI Wheel — What Good QI Actually Requires
QI is more than just running PDSA cycles. The RCGP QI Ready framework illustrates all the components that effective quality improvement depends on.
The Components of Effective Quality Improvement
It's not enough to just do PDSAs and mini-audits. Sustainable QI requires all of the following working together — like spokes on a wheel. Remove any one spoke and the wheel wobbles.
Learning Culture
QI only works in organisations where mistakes are discussed openly and learning is valued.
Patient Involvement
Listening to patient feedback identifies problems that professionals often miss entirely.
Stakeholder Engagement
Coercion delivers less than motivation. Get people on board — don't just issue instructions.
Evidence & Data
Trial and error gets hit-and-miss results. Base your changes on what the evidence says works.
Measurement
You cannot know if you've improved without measuring. Baseline + re-measure is non-negotiable.
PDSA / Testing
Test changes in small, safe cycles before implementing them across the whole system.
🔄 PDSA Cycles — The Engine of QI
PDSA (Plan, Do, Study, Act) is the most widely used QI methodology. Small, rapid cycles of testing and learning — not massive transformation attempts.
Plan
Define the change you want to test. Who, what, when, where? What do you predict will happen? Set up your measurement.
Do
Carry out the change on a small scale — a handful of patients, one week, one clinic session. Document what actually happens.
Study
Analyse what happened. Did it work as expected? What did you learn? Compare results to your prediction.
Act
Decide: adopt the change, adapt it, or abandon it. If it worked — scale it up. Start the next PDSA cycle.
- Small in scope — so manageable and safe
- Fast — you get results quickly
- Iterative — each cycle improves on the last
- Evidence-based — you test before scaling
- Team-friendly — everyone can engage
- Making the first cycle too large to manage
- Skipping the Study step — not analysing what happened
- Not measuring at all — no data = no QI
- Abandoning after one failure rather than adapting
- Doing it alone — PDSA is a team activity
🪜 Step-by-Step Guide to Your QIP
Here's exactly how to approach your Quality Improvement Project — from the first spark of an idea to submitting it on FourteenFish.
- Choose your topic wisely — Pick something that genuinely interests you AND has a clear practice need. The best topics are: something you've noticed isn't going well, a guideline you suspect isn't being followed, or a process that could be safer or more efficient.
- Define a clear, focused question — "Can we improve X in our practice?" — be specific. Avoid vague topics. A good title tells you exactly what is being measured.
- Review the evidence — What does NICE / the BNF / specialist guidance say? What standard are you measuring against? This is your "gold standard" for the audit criteria.
- Collect your baseline data — Search the clinical system. How are you currently performing against that standard? Record your numbers carefully — this is your "before."
- Identify the gap and the causes — Why is there a gap between what should happen and what is happening? Engage the team. Use a root cause analysis if helpful.
- Design and implement a change — What intervention will close the gap? Keep it practical and achievable. Run it as a PDSA cycle if it's a new or untested change.
- Re-measure after the intervention — Collect the same data again after a sufficient interval. Has performance improved? This is your "after."
- Reflect and document — What changed? What didn't? What would you do differently? What did you learn about working in teams and systems?
- Write it up and upload to FourteenFish — Complete the RCGP QIP template. Upload it to the dedicated QIP section on your FourteenFish ePortfolio (not the Learning Log).
- Discuss with your Educational Supervisor — Your ES will review, assess, and give graded feedback. This becomes evidence for your ARCP.
⚠️ Common Trainee Mistakes in QI
These are the patterns that repeatedly come up in supervisor feedback and ARCP reviews. Read them once and avoid them entirely.
-
❌
Treating SEA/LEA as a QIA Learning Event Analysis is a separate mandatory requirement and does NOT count as your annual QIA. Trainees discover this at their ARCP and it is not a pleasant surprise.
-
❌
Doing a QIP with no baseline data "I improved the template" is not a QIP without numbers. You must have before-and-after data. Even 10 cases is better than none.
-
❌
Leaving the QIP until ST3 ST3 is the year of the Leadership Project. Doing your QIP AND the Leadership Project in ST3 is overwhelming and avoidable. Do your QIP in ST1 or ST2.
-
❌
Choosing a secondary care QIP topic Your QIP must be relevant to primary care. A project done during a hospital post needs explicit agreement from your supervisor in advance.
-
❌
Writing a reflection without an action QIA requires action, not just reflection. "I noticed X and reflected on it" is not enough. "I noticed X, discussed with the team, changed protocol Y, and re-measured" is QIA.
-
❌
Uploading the QIP in the wrong place on FourteenFish The QIP goes in the dedicated QIP section of your FourteenFish ePortfolio — NOT in the Learning Log. These are different sections and the ARCP panel checks the right one.
-
❌
Doing a massive PDSA on the first cycle PDSA cycles are designed to be small and manageable. A cycle involving all 300 diabetic patients in the first test is not a PDSA — it's a full project. Start with 5–10 patients.
-
❌
Confusing audit with QI Audit is one type of QIA/QIP — not a synonym for all QI. Not all QI is audit. This matters when your supervisor asks: "What type of QI activity is this?"
💎 Insider Wisdom — What Trainees Actually Say
Hard-won insights distilled from UK GP registrar experience, deanery trainee forums, and peer-to-peer training community knowledge. All consistent with RCGP and GMC guidance.
🔑 The Things Nobody Puts in the Official Handbook
Your QIP write-up matters as much as the project itself. QIPs are regularly rejected at ARCP not because the project was bad — but because the reflection was thin. Write as you go. Don't try to reconstruct the whole journey at the end from memory.
The RCGP explicitly says to keep QIPs "simple and small scale." Trainees consistently over-scope and then run out of time. A focused prescribing review of 15 patients, done properly with two PDSA cycles, impresses supervisors far more than an ambitious practice-wide overhaul that never quite finished.
Practice managers can pull data searches from EMIS or SystmOne that you didn't know were possible — often in minutes. They also know which problems have been nagging the practice for months, which makes for excellent, practice-relevant QIP material. They are your most underused QI asset.
"Who maintains this when you leave?" is a standard ARCP discussion point. A QIP that changes a system, creates a template, or updates a protocol is far more sustainable than one that relies on a single motivated individual (i.e. you) being present. Build the answer into your design.
⚠️ What Actually Gets QIA Entries Rejected at ARCP
These patterns come up repeatedly in deanery ARCP panel feedback. Knowing them in advance saves considerable stress.
-
⚠️
Reflection without action The most common rejection reason. "I reviewed my last 20 prescriptions and noticed I tend to prescribe X" — that's not a QIA. A QIA must show: data → finding → action → what changed as a result. Even a small change counts. No change = no QIA.
-
⚠️
No personal connection to the work The RCGP requires the QIA to involve "a personal connection to a registrar's work." Reviewing a national audit your practice participated in, without any personal involvement in data collection or change, does not meet the criteria.
-
⚠️
Simply reviewing consultations without structure Casually reflecting on some of your recent consultations — however thoughtful — is not a QIA. There must be systematic data collection, comparison to a standard or benchmark, and documented action taken as a result.
-
⚠️
QIP uploaded in the Learning Log instead of the QIP section This sounds trivial. It is not. ARCP panels check the dedicated QIP section of FourteenFish. A QIP filed as a Learning Log entry may not be found or counted. Always use the correct section.
-
⚠️
QIP not assessed by supervisor Your supervisor must have assessed and rated your QIP on the FourteenFish form, with all sections completed. An unassessed QIP is an incomplete QIP, regardless of how good the project was. Chase this up before your ARCP deadline.
-
⚠️
A QIP that only discusses change rather than implementing it The RCGP explicitly flags this as a common indicator of an unsatisfactory QIP: "No real attempt at implementing change, just a discussion that change should happen." Data collection + presentation of findings ≠ quality improvement. You must actually make a change happen.
🌟 What Supervisors and ARCP Panels Actually Love
These are the things that consistently earn strong assessments — drawn from assessor feedback and deanery guidance.
-
✅
Honest reporting when things didn't improve A write-up that thoughtfully explains why improvement wasn't achieved, what barriers existed, and what you learned is excellent QI work. Supervisors are more suspicious of suspiciously dramatic improvement with no struggle than of honest, reflective non-improvement.
-
✅
Evidence of team engagement Did you present findings at a practice meeting? Did you involve the reception team, nursing staff, or pharmacist? Projects that demonstrate real team engagement — not just mentioning "I spoke to the team" — score consistently higher.
-
✅
Run charts over static tables A run chart (data plotted over time as a line graph) shows change dynamically and is far more compelling than a before/after table. RCGP guidance explicitly recommends run charts. They demonstrate QI thinking, not just data collection. Free run chart tool available at the IHI website.
-
✅
Two or more PDSA cycles The RCGP QIP guidance specifies that QIPs should include at least two PDSA cycles. Projects with only one cycle — "we made a change and re-measured" — are less complete than those showing iteration and learning from the first cycle before running a second.
-
✅
A clear personal narrative — what you specifically did Assessors want to see your individual contribution clearly separated from what the team did collectively. Use first-person language. "I collected the baseline data, I designed the template, I presented at the practice meeting" — this is what makes your involvement legible on the page.
-
✅
Reflection on what you would do differently next time The "what will I maintain, improve, or stop?" structure (from the RCGP marking rubric) is your friend. Assessors look for honest self-evaluation. Candidates who can critically appraise their own QI work demonstrate significantly higher competence than those who simply summarise what happened.
🎯 How to Pick a Topic That Won't Cause Problems
Choosing the wrong topic is the most avoidable QIP mistake. Use this filter before committing.
🚫 Topics That Tend to Cause Trouble
✅ Topics That Tend to Work Well
✍️ Writing Up Your QIP — What Actually Works
Structure your write-up around the RCGP's own marking domains
The QIP template asks you to describe: (1) why you chose the topic and the evidence base, (2) what tools you used to understand the problem, (3) what data you collected and how, (4) what change you made and how you measured impact, (5) how you engaged the team and stakeholders, and (6) what you learned and what you'd do differently. Write explicitly to each of these — assessors mark against them directly.
Give your QIP a specific, unambiguous title
Compare: "Improving diabetes care" vs "Improving HbA1c documentation rates at annual review in patients with Type 2 Diabetes at [Practice Name]." The second title tells the assessor exactly what was measured, in whom, where, and why it matters. A specific title signals a focused, well-designed project before they've read a single line.
Write contemporaneously — not in a rush at the end
Document each PDSA cycle as you do it. Note down what you predicted, what happened, what surprised you. These real-time observations make for much richer, more credible reflection than trying to reconstruct your thought process weeks later. Portfolio entries backdated and uploaded all at once are visible to assessors — the date-shared field on FourteenFish shows when entries were actually added.
Use the "what will I maintain, improve, or stop?" framework
This three-part closing reflection is specifically referenced in the RCGP QIP feedback guidance. It demonstrates that you can critically evaluate your own QI methodology, not just report what happened. Even if your intervention was successful, there is always something you'd do differently — and saying so honestly impresses assessors far more than claiming everything was perfect.
LTFT trainees can absolutely complete a QIP — but allow extra time. A QIP intended for a 4–6 month GP post may take proportionally longer in a LTFT post. Discuss timing early with your ES so that the post is long enough to complete both PDSA cycles before your placement ends. Don't start a QIP in your final few weeks of a post.
Many deaneries run facilitated peer groups for trainees working on QIPs. Evidence from GP training guidance consistently shows that trainees who use peer groups produce better projects and find the process significantly less stressful. Other registrars may have tried QI tools you haven't encountered, solved problems similar to yours, or identified resources that made the difference. Ask your TPD or programme manager whether there's a group running in your deanery.
Insights synthesised from UK deanery trainee guidance, ARCP panel feedback, GP registrar accounts, and GP training community resources. All consistent with current RCGP and GMC requirements.
🎓 For Trainers — Teaching QI Effectively
Common blind spots, tutorial ideas, and reflective prompts for educational supervisors and GP trainers teaching QI.
📌 Trainer Guidance for QI
- Confusing SEA/LEA with QIA — many trainees believe they've completed their QIA by doing a learning event analysis
- Not understanding the difference between QIA and QIP — often assume they're the same thing at different scales
- Treating QI as a paperwork exercise rather than genuine improvement
- Not measuring — writing a reflective piece without any data
- Choosing a topic that is too broad ("improving diabetes care in our practice") rather than focused ("improving foot examination rates at annual review")
- Not involving the team — attempting QI in isolation
- Ask the trainee to describe a time they noticed something could be done better in the practice — then trace it through the 3 fundamental questions framework together
- Walk through the Donabedian model using a clinical example from their own experience
- Design a mock PDSA cycle together for a simple problem — helps trainees understand the practical steps
- Review a completed QIP from the RCGP website or Bradford VTS examples — ask what was done well and what could be improved
- Ask: "What would a QIA look like for your prescribing this week?" — encourages habitual QI thinking
- "What does 'quality' mean to you in your day-to-day practice?"
- "What's one thing you've noticed this week that could be done better — and what's stopping it from being better?"
- "If you had to measure the quality of your own prescribing, how would you do it?"
- "How would a patient describe the quality of your consultation with them last week?"
- "What would you do differently if you knew you were being audited?"
- "Tell me about a time when a small change in your practice made a real difference to a patient."
- Ask trainees to bring their QIA reflections to tutorials — discuss not just what they did, but what they changed as a result
- Check that the QIP includes baseline data, intervention, and re-measurement — without all three, it's incomplete
- Look for team engagement in the write-up — a solo QIP that ignores the wider team misses an important learning opportunity
- Assess understanding of measurement — "How would you know if your change actually worked?"
- Ensure the FourteenFish upload is in the correct QIP section (not the Learning Log)
🙋 FAQ — The Questions Everyone Asks
Practical answers to the questions that come up again and again.
✅ Final Take-Home Points
⭐ The Bits to Remember Tomorrow
- QI is about moving to a better place — not proving you're already there
- QA = for others. QI = for you, your team, and your patients
- You need 1 QIP + 2 QIAs by end of ST3 — do the QIP in ST1 or ST2
- QIP lives in the dedicated FourteenFish QIP section — NOT the Learning Log
- SEA/LEA does NOT count as your QIA — they are separate requirements
- Every QI project answers: What am I trying to achieve? How will I measure it? What change will I test?
- Donabedian: Structure → Process → Outcome — always think in this framework
- PDSA: Plan, Do, Study, Act — start small, measure, build upwards
- No measurement = no QI. Always have a before and an after
- The RCGP QI Ready Toolkit is free, excellent, and underused — use it
QI Activities
QI Tools (to be developed)
What is Quality Improvement?
Quality Improvement (QI) is an evidence-based approach that helps primary care free up time to deliver and evaluate initiatives, and embed new approaches more effectively and efficiently into practice. QI helps us to make the most of our systems, organisations, talents and expertise to deliver better outcomes for patients.
The QI Wheel
I love this diagram of the QI Wheel (found the on the RCGP’s QI Ready Online Toolkit). Why?
- Because it illustrates all the components of good QI work.
- And then it brings all of it together as a cohesive whole
- And it’s based on evidence.
To go into more detail…. it’s not just about doing lots of PDSAs, Significant Events or mini-audits! None of that works if…
- You don’t belong to a working organisation whose has a good learning culture in place.
- You don’t involve or listen to patients when they complain something is not delivering good quality of care.
- You don’t engage the other stakeholders in a meaningful way (i.e. for example, if you force someone to do a task because your their boss, you are likely to get less quality results than someone who is as near passionate about it as you are).
- You don’t base it on what the evidence and research says that makes a difference. If you just do stuff by trial and error, you get hit and miss results (more miss actually).