ENT for GPs: Your Essential Guide
From earwax to epiglottitis - because every GP needs to know when to worry and when to wax lyrical about wax removal
Last Updated: March 2026
Executive Summary: What You'll Master Today
Because you have 47 other things to do before lunch, and that's just the morning list
What This Page Covers:
Quick Facts at a Glance:
Downloads
path: EAR, NOSE & THROAT
- A Generalists Guide to ENT.pptx
- Audiometry Interpretation.pdf
- BPPV - Hallpike Epleys Manouvre.pdf
- Ear Conditions in GP 1.pptx
- Ear Conditions in GP 2.pptx
- Eardrums.pptx
- Easy Peasy Eardrums.ppt
- ENT core curriculum for GP trainees.docx
- ENT Emergencies in GP.pptx
- ENT in pictures 1.pdf
- ENT in pictures 2.pdf
- Normal Ear & Surface Anatomy.ppt
- Obstructive Sleep Apnoea & Snoring.pptx
- Sinusitis and Rhinosinusitis.pptx
- TEACHING - Acoustic Neuroma OSCE Station.docx
- TEACHING - dental problems.doc
- TEACHING - osa case.doc
- TEACHING - sinusitis case.doc
- Tinnitus.pptx
- Vertigo and BPPV.pptx
Web Resources
- RCGP ENT Curriculum Topic Guide ↗ Outlines what a GP trainee should know and do in ENT, covering red flags, common presentations, and learning suggestions aligned to WPBAs and AKT.
- Hull University Teaching Hospitals — Primary Care ENT Guidance ↗ Pragmatic initial management of common ENT conditions agreed jointly by ENT specialists and primary care clinicians.
- North West London ICB — ENT Primary Care Guidance ↗ Primary-care-oriented guidance and referral criteria for common ENT presentations from NW London ICB.
- GIRFT ENT Referral Guidelines — Adults (PDF) ↗ National standardised referral pathways from primary care for adult ENT presentations, with suggested work-up and referral content guidance.
- GIRFT ENT Referral Guidelines — Paediatrics (PDF) ↗ As above for children, with paediatric-specific indications, safety-netting advice, and clear referral criteria.
- ENTSHO.com ↗ Concise on-call-style pages covering otitis externa/media, epistaxis, quinsy, stridor and more — practical management steps and red flags, very GP-usable.
- ENT UK — Community & GP Resources ↗ Hosts clinical guidelines, patient leaflets, and the practical Official Handbook for Medical Students and Junior Doctors — useful for GP trainees.
- ENT UK — GPwER Guidance (PDF) ↗ Knowledge, skills, and training expectations for GPs with an Extended Role in ENT — useful for those building a community ENT service.
- ENT UK — "What Should a GP Learn About ENT?" (PDF) ↗ Core ENT knowledge and skills benchmarked for GPs — useful when planning GP training sessions or a self-study plan.
Equipment Required
- Otoscope
- Specula (various sizes)
- Pneumatic attachment (optional)
Examination Steps
Normal Findings
- Pearly grey tympanic membrane
- Cone of light at 5 o'clock (right) or 7 o'clock (left)
- Visible malleus handle
- Mobile membrane with pneumatic insufflation
Abnormal Findings
- Red, bulging membrane (acute otitis media)
- Retracted membrane with visible fluid level (otitis media with effusion)
- Perforation
- Cholesteatoma (white debris, attic perforation)
- Wax impaction
- Otitis externa (canal inflammation)
Equipment Required
- 512 Hz tuning fork
Examination Steps
Normal Findings
- Rinne positive: Air conduction > bone conduction (AC>BC)
- Weber: Sound heard equally in both ears (midline)
Abnormal Findings
- Conductive loss: Rinne negative (BC>AC), Weber lateralizes to affected ear
- Sensorineural loss: Rinne positive, Weber lateralizes to better ear
- Mixed loss: Rinne may be negative, Weber lateralizes to better ear
Equipment Required
- Examination couch
- Frenzel glasses (optional)
Examination Steps
Normal Findings
- No nystagmus
- No vertigo
Abnormal Findings
- BPPV: Rotatory nystagmus after 5-10 second latency
- Nystagmus fatigues with repeated testing
- Vertigo accompanies nystagmus
- Central causes: Immediate nystagmus, no latency, no fatigue
Equipment Required
- Thudichum nasal speculum
- Light source
- Decongestant spray (optional)
Examination Steps
Normal Findings
- Pink, moist mucosa
- Midline septum
- Visible inferior turbinate
- No discharge or polyps
Abnormal Findings
- Septal deviation
- Nasal polyps (pale, grape-like)
- Mucopurulent discharge (sinusitis)
- Mucosal inflammation (rhinitis)
- Epistaxis source
- Foreign body
Equipment Required
- Tongue depressor
- Light source
- Gloves
Examination Steps
Normal Findings
- Pink, moist mucosa
- Symmetrical tonsils
- No exudate
- Midline uvula
- No ulceration
Abnormal Findings
- Tonsillar exudate (bacterial tonsillitis)
- Asymmetric tonsils (quinsy, malignancy)
- Petechiae on palate (EBV)
- Ulceration (aphthous, malignancy)
- Candidiasis (white plaques)
- Deviated uvula (quinsy)
Equipment Required
- None required
Examination Steps
Normal Findings
- No visible swelling
- No palpable lymph nodes (or small, soft, mobile nodes)
- Symmetrical neck movement
Abnormal Findings
- Lymphadenopathy: size, consistency, mobility, tenderness
- Thyroid enlargement
- Neck mass (branchial cyst, thyroglossal cyst, malignancy)
- Supraclavicular nodes (high risk of malignancy)
Key History Questions
- Onset and duration?
- Unilateral or bilateral?
- Associated hearing loss or discharge?
- Recent URTI or swimming?
- Pain on moving jaw or pulling pinna?
- Systemic symptoms (fever)?
Examination Findings to Look For
- Otoscopy: TM appearance, perforation, discharge
- Pinna and canal examination
- Mastoid tenderness
- TMJ examination
- Throat examination (referred pain)
Investigations
- Usually clinical diagnosis
- Swab if otorrhoea present
- Imaging if mastoiditis suspected
Differential Diagnoses
Key History Questions
- Sudden or gradual onset?
- Unilateral or bilateral?
- Associated tinnitus or vertigo?
- Noise exposure history?
- Family history of hearing loss?
- Ototoxic medications?
Examination Findings to Look For
- Otoscopy: wax, perforation, effusion
- Rinne and Weber tests
- Whispered voice test
- Cranial nerve examination if unilateral
Investigations
- Audiometry (pure tone and speech)
- Tympanometry
- MRI IAM if unilateral SNHL
- Blood tests if sudden SNHL (FBC, ESR, glucose)
Differential Diagnoses
Key History Questions
- True vertigo (spinning) or dizziness?
- Duration of episodes?
- Triggers (head movement, position)?
- Associated hearing loss or tinnitus?
- Neurological symptoms?
- Headache or visual disturbance?
Examination Findings to Look For
- Dix-Hallpike test
- Gait and Romberg test
- Cranial nerve examination
- Nystagmus assessment
- Cardiovascular examination (postural BP)
Investigations
- Usually clinical diagnosis for BPPV
- Audiometry if Ménière's suspected
- MRI brain if central cause suspected
- ECG if cardiac cause suspected
Differential Diagnoses
Key History Questions
- Unilateral or bilateral?
- Constant or intermittent?
- Associated rhinorrhoea or sneezing?
- Seasonal variation?
- Epistaxis or blood-stained discharge?
- Facial pain or pressure?
Examination Findings to Look For
- Anterior rhinoscopy
- Assess for polyps, septal deviation
- Facial tenderness (sinusitis)
- Lymphadenopathy
Investigations
- Usually clinical diagnosis
- CT sinuses if chronic rhinosinusitis
- Allergy testing if allergic rhinitis
- Nasal endoscopy if unilateral symptoms
Differential Diagnoses
Key History Questions
- Duration of symptoms?
- Fever or systemic upset?
- Difficulty swallowing or breathing?
- Cough or coryzal symptoms?
- Contact with streptococcal infection?
- Immunization status (diphtheria)?
Examination Findings to Look For
- Throat examination: tonsillar exudate, symmetry
- Cervical lymphadenopathy
- Temperature
- Respiratory rate and effort
- Trismus or drooling
Investigations
- FeverPAIN or Centor score
- Throat swab if recurrent
- Monospot if EBV suspected
- Imaging if quinsy suspected
Differential Diagnoses
| Location | Inflammatory | Structural | Neoplastic |
|---|---|---|---|
| External Ear | Otitis externa, Perichondritis | Wax impaction, Foreign body | SCC, BCC |
| Middle Ear | AOM, OME, Mastoiditis | Cholesteatoma, Perforation | Glomus tumour |
| Inner Ear | Labyrinthitis, Vestibular neuronitis | BPPV, Ménière's | Acoustic neuroma |
| Nose/Sinuses | Rhinitis, Sinusitis | Polyps, Septal deviation | Nasal carcinoma |
| Throat | Pharyngitis, Tonsillitis, Quinsy | Tonsillar hypertrophy | Oropharyngeal carcinoma |
| Larynx | Laryngitis, Epiglottitis | Vocal cord nodules/polyps | Laryngeal carcinoma |
Clinical Features — Pharyngitis & Tonsillitis
- Sore throat, odynophagia, fever
- Viral cause in ~70% — coryzal symptoms, no exudate
- Bacterial (Group A Strep) — tonsillar exudate, fever >38°C, no cough, lymphadenopathy
- EBV (glandular fever) — splenomegaly, generalised lymphadenopathy, palatal petechiae
- FeverPAIN score: Fever, Purulence, Attend rapidly (<3 days), Inflamed tonsils, No cough
- Recurrent tonsillitis: ≥7 episodes/year, ≥5/year for 2 years, or ≥3/year for 3 years (Paradise criteria)
⚠️ Clinical Features — Quinsy (Peritonsillar Abscess)
- Severe unilateral throat pain — dramatically worse than typical tonsillitis, often can barely swallow
- "Hot potato" muffled voice — classic, immediately recognisable
- Trismus (difficulty opening the mouth) — due to pterygoid muscle spasm
- Uvular deviation away from the affected side — hallmark sign
- Visible bulge of the soft palate and tonsil on the affected side, pushing the tonsil medially
- Drooling (unable to swallow saliva), high fever, systemically unwell
- Usually follows 4-7 days of worsening tonsillitis — patient feels "this is different, much worse"
The case for watchful waiting
Around 80% of sore throats are viral and self-limiting. Even when bacterial (Streptococcus pyogenes), the infection is often self-limiting and antibiotics shorten symptoms by only about half a day. Reserve antibiotics for higher FeverPAIN/Centor scores.
💬 What to say to patients / parents:
"Most sore throats settle within a week. Antibiotics only shorten things by about half a day. The throat is usually worst around day 3 or 4, then gradually improves day by day."
For parents: "If little Johnny had a twin and we gave Johnny antibiotics but nothing to the twin, they'd both usually be better by day 7. The antibiotic might just make Johnny better half a day earlier."
🦠 Classic viral clues
- • Cough
- • Coryza / runny nose
- • Conjunctivitis
- • Hoarseness
- • Diarrhoea
🔴 Classic bacterial clues
- • Fever
- • Tonsillar exudate
- • Tender anterior cervical lymphadenopathy
- • Absence of cough
Immediate Management
- Analgesia — paracetamol and ibuprofen regularly
- Encourage fluids and rest
- Calculate FeverPAIN or Centor score
- If quinsy suspected — same-day ENT referral for incision & drainage
Primary Care Management — Pharyngitis/Tonsillitis
- FeverPAIN 0-1: no antibiotics
- FeverPAIN 2-3: delayed antibiotic prescription
- FeverPAIN ≥4: phenoxymethylpenicillin 500mg QDS × 10 days (first-line)
- Penicillin allergy: Clarithromycin 250mg twice daily × 5 days (adults)
- Never give amoxicillin if EBV suspected — causes widespread maculopapular rash
- Monospot test if EBV suspected — advise no contact sport for 3-4 weeks (splenic rupture risk)
- Safety net: return if worsening, drooling, trismus, difficulty breathing or swallowing
⚠️ Why not amoxicillin?
1️⃣ Rash risk in EBV
Up to 90% of patients with infectious mononucleosis develop a widespread maculopapular rash if given amoxicillin. It's not a true allergy, but it's alarming for patients and creates lasting confusion about penicillin allergy. Phenoxymethylpenicillin carries far lower risk of triggering this reaction.
2️⃣ Antimicrobial stewardship
Phenoxymethylpenicillin is narrow-spectrum — it targets Streptococcus pyogenes (Group A strep) precisely. Amoxicillin is broader-spectrum, which promotes resistance and disrupts normal flora unnecessarily. Use the narrowest effective agent.
Quinsy — Management
- Same-day ENT referral — incision and drainage (I&D) or aspiration under local anaesthetic
- IV antibiotics and fluids if systemically unwell or unable to swallow
- IV dexamethasone to reduce swelling and speed recovery
- Interval tonsillectomy considered after second quinsy
- Do NOT attempt to lance or examine aggressively in primary care
ENT Referral — Tonsillectomy
- Paradise criteria met: ≥7 episodes in 1 year, OR ≥5/year for 2 years, OR ≥3/year for 3 years; each with fever >38.3°C, cervical lymphadenopathy, tonsillar exudate, or positive strep
- Obstructive sleep apnoea from tonsillar hypertrophy
- Recurrent quinsy — interval tonsillectomy
- Unilateral tonsillar enlargement without infection — 2WW malignancy referral
Red Flags - Urgent Action Required
- Hot potato voice + trismus + uvula deviation + visible palatal bulge = Quinsy — same-day ENT
- Stridor or airway compromise — call 999 immediately, do not examine throat
- Neck stiffness with sore throat — meningitis
- Unilateral tonsillar enlargement without acute infection — malignancy, 2WW referral
- Drooling with inability to swallow — airway at risk, emergency
- Severe systemic sepsis — admit urgently
- Epiglottitis — drooling, inspiratory stridor, unable to swallow, sitting forward, muffled voice: DO NOT EXAMINE THROAT, call 999, keep child calm
- Respiratory distress or stridor — airway emergency, call 999
- Severe dysphagia — unable to swallow saliva, drooling: admit urgently
Clinical Features
- Ear pain (otalgia)
- Fever and systemic upset
- Bulging, red tympanic membrane
- Reduced hearing
- Otorrhoea if perforation occurs
Immediate Management
- Analgesia (paracetamol/ibuprofen)
- Safety-netting advice
Primary Care Management
- Watchful waiting for 72 hours in most cases
- Delayed antibiotic prescription
- Immediate antibiotics if: systemically unwell, <2 years with bilateral AOM, otorrhoea, immunocompromised
- First-line: Amoxicillin 500mg three times daily × 5 days (adults; 7 days if severe)
- Second-line / penicillin allergy: Clarithromycin 500mg twice daily × 5 days; or if treatment failure: Co-amoxiclav 500/125mg three times daily × 5–7 days
Specialist Referral Indications
- Recurrent AOM (≥4 episodes in 6 months)
- Persistent effusion >3 months
- Complications (mastoiditis, intracranial)
Red Flags - Urgent Action Required
- Severe systemic infection
- Mastoiditis (post-auricular swelling, tenderness)
- Meningitis symptoms
- Facial nerve palsy
Clinical Features
- Conductive hearing loss, often bilateral
- Speech and language delay in young children
- Inattentiveness at school — often first noticed by teachers
- Recurrent ear infections in some cases
- Dull, retracted or fluid-filled tympanic membrane on otoscopy
- Flat tympanogram (type B) on tympanometry
- Hearing loss ≥25dB in better ear — threshold for intervention
- OME persisting >3 months despite conservative management
- Impact on speech, language, development or learning
Immediate Management
- Reassurance — most cases resolve spontaneously within 3 months
- Watchful waiting with hearing monitoring
- Formal audiology referral — pure tone audiogram
- Document any impact on learning, behaviour or development
Primary Care Management
- Watchful waiting for 3 months before referral in most cases
- Autoinflation (Otovent balloon) — encourage twice daily use
- Treat any underlying allergic rhinitis contributing to Eustachian tube dysfunction
- Refer to audiology for hearing assessment
- Advise parents to minimise exposure to passive smoke
Specialist Referral Indications
- Persistent bilateral OME >3 months with hearing loss
- Speech, language or developmental concerns
- Significant impact on quality of life or education
- Recurrent AOM with effusion between episodes
Red Flags - Urgent Action Required
- Significant speech or language delay — urgent audiology referral
- Suspected cholesteatoma — white debris, attic perforation
- Unilateral OME in adults — must exclude nasopharyngeal carcinoma
- Associated craniofacial abnormality (e.g. Down syndrome, cleft palate)
- Frequent AOM causing significant morbidity — expedite ENT referral
- Educational concerns raised by school or parents — prioritise referral
Clinical Features
- Chronic ear discharge >6 weeks
- Through perforated tympanic membrane
- Often painless (unlike acute otitis media)
- May have conductive hearing loss
- Offensive smell common
Immediate Management
- Aural toilet (gentle cleaning/suction)
- Keep ear dry - avoid water
Primary Care Management
- First-line: Ciprofloxacin 0.3% ear drops — 4 drops into affected ear twice daily × 7 days (NICE first choice for perforated drum)
- Second-line: Ofloxacin 0.3% ear drops — 10 drops into affected ear once daily × 7 days
- 7-14 days treatment
- More effective than oral antibiotics
- Review in 2 weeks
Specialist Referral Indications
- No improvement after 4-6 weeks of treatment
- Recurrent episodes despite treatment
- Suspected cholesteatoma (foul smell, hearing loss)
- Complications (facial nerve palsy, vertigo, headache)
Red Flags - Urgent Action Required
- Facial nerve palsy
- Vertigo or balance problems
- Severe headache
- Signs of intracranial complications
👂 Vestibular Neuronitis
The vestibular nerve — the nerve that carries balance signals from the inner ear to the brain — becomes inflamed, usually after a viral illness. The cochlea (hearing part) is completely unaffected.
Think of it as the balance signal cable going down — the brain suddenly gets no balance input from one side, causing intense spinning vertigo. It's like pulling the plug on one side of a stereo balance system.
👉 Hearing is normal — the cochlear nerve is untouched.
🦠 Labyrinthitis
Inflammation spreads into the labyrinth itself — the fluid-filled bony structure that houses both the vestibular apparatus (balance) and the cochlea (hearing). Usually viral, occasionally bacterial (rare but serious).
Because both systems are involved, patients get vertigo and hearing loss. The vertigo is just as severe as vestibular neuronitis, but the added cochlear damage is the distinguishing feature.
👉 Hearing loss is present — this is the key difference.
| Vestibular Neuronitis | Labyrinthitis | |
|---|---|---|
| Structures affected | Vestibular nerve only | Labyrinth (cochlea and vestibular apparatus) |
| Vertigo | Severe, constant, sudden onset | Severe, constant, sudden onset |
| Hearing loss | ❌ None — hearing preserved | ✅ Present — often significant |
| Tinnitus | Absent | Often present |
| Nystagmus | Horizontal, fast phase away from affected side | Horizontal, fast phase away from affected side |
| Preceding illness | Often post-viral URTI (presumed viral neuritis) | Often post-viral or during acute viral illness |
| Duration of acute phase | Days to 2–3 weeks of severe symptoms | Days to 2–3 weeks of severe symptoms |
| Full recovery | Weeks to months; most recover fully; some residual imbalance | Weeks to months; hearing loss may be permanent |
| HiNTS exam | Peripheral pattern (reassuring) | Peripheral pattern (reassuring) |
🧠 The key differentiator
Hearing loss = Labyrinthitis. No hearing loss = Vestibular neuronitis. Both cause continuous severe vertigo lasting days — unlike BPPV (seconds) or Ménière's (hours). Both are peripheral vestibular disorders and should not show neurological signs.
The HINTS Examination
Use HINTS (Head impulse, Nystagmus, Test of Skew) in patients presenting with acute continuous vertigo with nystagmus within hours or days of onset to differentiate peripheral (e.g. vestibular neuritis) from central (e.g. posterior circulation stroke). Do not use for intermittent vertigo (e.g. BPPV).
✅ Reassuring — likely peripheral (e.g. vestibular neuritis)
- Head impulse: Abnormal — catch-up saccade present (eyes lag then correct)
- Nystagmus: Unidirectional horizontal — beats in one direction only
- Test of Skew: No vertical skew — eyes stay level on alternate cover test
⚠️ Worrying — possible central cause (stroke/tumour) — needs imaging
- Head impulse: Normal — no catch-up saccade (eyes stay on target despite head movement)
- Nystagmus: Bidirectional or vertical — direction changes with gaze, or beats vertically
- Test of Skew: Vertical skew present — one eye higher than the other on alternate cover
📅 Recovery timeline (both conditions)
- Day 1–3: Worst phase — severe constant vertigo, unable to stand or walk safely, nausea and vomiting
- Day 3–7: Gradual improvement; vertigo less constant but still provoked by movement
- Week 2–6: Central compensation begins; symptoms gradually resolve; imbalance improves
- 3–6 months: Most patients fully compensated; some have residual imbalance, especially in the elderly
Immediate Management
- Reassure — benign peripheral vestibular disorder, will resolve
- Advise bed rest during the acute phase (day 1–3); avoid driving
- Hydration — IV fluids if unable to tolerate oral fluids due to vomiting
- If labyrinthitis with significant hearing loss: urgent ENT referral to exclude sudden SNHL requiring steroids
Vestibular Sedatives — Short-term only (max 3–7 days)
- First-line — antihistamine (vestibular sedative): Cinnarizine 30mg three times daily (unlicensed but widely used in UK practice); or Promethazine 25mg twice daily — max 7 days
- Second-line — phenothiazine antiemetic: Prochlorperazine 3–6mg buccal (Buccastem) twice daily, or 5mg orally three times daily, or 12.5mg IM if vomiting severely — max 7 days
- Alternative antiemetic: Metoclopramide 10mg three times daily (short-term); or Ondansetron 4–8mg twice daily for refractory nausea
Vestibular Rehabilitation
- Encourage mobilisation as soon as tolerated — movement promotes vestibular compensation
- Vestibular rehabilitation exercises (Cawthorne-Cooksey exercises) — begin once acute phase settles, usually week 2
- Formal vestibular physiotherapy referral if symptoms persist beyond 6 weeks
- AVOID prolonged vestibular sedatives — they impair central compensation
Specialist Referral Indications
- Any associated hearing loss — ENT urgently (exclude sudden SNHL)
- Neurological symptoms (diplopia, dysarthria, dysphagia, ataxia, facial palsy) — emergency neurology/stroke
- Symptoms not improving after 6 weeks — ENT or neurology
- Recurrent episodes — consider Ménière's disease, vestibular migraine
- Diagnostic uncertainty — atypical nystagmus, no preceding viral illness
Red Flags - Urgent Action Required
- Neurological symptoms (diplopia, dysarthria, dysphagia, facial palsy, limb ataxia) — posterior circulation stroke until proven otherwise, emergency 999
- Direction-changing nystagmus, vertical nystagmus, or nystagmus that does not suppress with fixation — central cause, urgent neurology
- Severe headache with acute vertigo — subarachnoid haemorrhage or posterior fossa bleed
- Associated hearing loss with acute vertigo — labyrinthitis; if sudden SNHL, urgent ENT for steroids within 2 weeks
- Truncal ataxia — unable to sit unaided; suggests central pathology
- New onset vertigo in patient with vascular risk factors (hypertension, diabetes, atrial fibrillation) — higher index of suspicion for posterior circulation stroke
🌼 UK Pollen Season Calendar
🌳 Tree pollen
March – May
🌾 Grass pollen
May – July (peak)
🍂 Weed/mould
July – September
Clinical Features
- Sneezing — often paroxysmal, triggered by pollen exposure
- Clear watery rhinorrhoea
- Nasal congestion and itching
- Itchy, red, watery eyes (allergic conjunctivitis) — present in ~70% of cases
- Itchy palate and throat
- Reduced smell and taste during episodes
- Fatigue — underappreciated; significantly impacts quality of life, school and work performance
- Symptoms clearly seasonal — correlate with pollen count
- Worsened by outdoor exposure, warm windy days, fresh-cut grass
- Associated asthma: 30–40% of hayfever patients have asthma — always ask about chest symptoms
📊 Stepwise approach — match treatment to severity
Start 2 weeks before the anticipated season begins for best effect. Step up if symptoms not controlled after 2–4 weeks at each level.
Step 1 — Mild intermittent symptoms
- Drug class: Non-sedating oral antihistamine
- First-line: Cetirizine 10mg once daily — taken as needed or regularly during season (OTC, inexpensive, effective)
- Alternative: Loratadine 10mg once daily (marginally less sedating than cetirizine in some patients)
- Alternative: Fexofenadine 120mg once daily — truly non-sedating; useful for drivers, pilots, those operating machinery
- Add: Topical antihistamine eye drops if conjunctivitis prominent — Sodium cromoglicate 2% eye drops 1–2 drops 4 times daily, or Azelastine 0.05% eye drops 1 drop twice daily
Step 2 — Moderate / persistent symptoms
- Drug class: Intranasal corticosteroid (INCS) — most effective single treatment for nasal symptoms
- First-line INCS: Fluticasone propionate 2 sprays (100 micrograms) per nostril once daily — start 2 weeks before season; continue throughout season
- Alternative INCS: Mometasone furoate 2 sprays (100 micrograms) per nostril once daily — equivalent efficacy, slightly different particle size
- Alternative INCS: Beclometasone dipropionate 2 sprays (100 micrograms) per nostril twice daily
- Continue oral antihistamine alongside INCS if eye or skin symptoms persist
- Drug class: Intranasal antihistamine (adjunct) — Azelastine 0.14% nasal spray 1 spray per nostril twice daily — fast-acting (15 min), useful for breakthrough symptoms
Step 3 — Severe / poorly controlled symptoms
- Drug class: Combined intranasal antihistamine + corticosteroid
- First-line combination: Azelastine / Fluticasone propionate (Dymista) 1 spray per nostril twice daily — more effective than either component alone; NICE-approved
- Drug class: Leukotriene receptor antagonist — add if asthma coexists
- Add-on for asthma + hayfever: Montelukast 10mg once daily at night — especially useful when both conditions co-exist
- Nasal decongestant (short-term only): Xylometazoline 0.1% — 1–2 sprays per nostril up to 3 times daily, maximum 7 days. Do not exceed 7 days — risk of rhinitis medicamentosa (rebound congestion)
Step 4 — Very severe / debilitating / exam-season crisis
- Drug class: Short course oral corticosteroid
- First-line oral steroid rescue: Prednisolone 20–25mg once daily in the morning × 5–7 days — for acute severe exacerbation or exam crisis; no taper needed for courses <2 weeks
- Important: Avoid IM triamcinolone (Kenalog) injection — not recommended by BSACI/NICE due to risk of adrenal suppression, avascular necrosis of hip, and prolonged systemic steroid exposure. Oral prednisolone is safer and controllable
- Drug class: Intranasal corticosteroid — escalated dose
- Ensure Dymista is optimised (step 3) before prescribing oral steroids
- Concurrent asthma flare: Review and step up inhaled corticosteroid therapy; refer to asthma nurse/GP asthma review if poorly controlled during season
Step 5 — Allergen immunotherapy (specialist)
- Drug class: Allergen immunotherapy (subcutaneous or sublingual)
- Sublingual immunotherapy (SLIT): Grazax (grass pollen) — 75,000 SQ-T grass allergen tablet dissolved under tongue once daily, started 4 months before season, continued for 3 years
- Alternative SLIT: Actair or Staloral — taken daily, long-term (3 years minimum)
- Refer to allergy clinic / immunologist for assessment — indicated for patients with confirmed grass or tree pollen allergy failing maximum pharmacotherapy
- SLIT significantly reduces symptom burden and medication use; may modify disease course long-term
Non-pharmacological measures (reinforce at every step)
- Check pollen count daily (Met Office app or BBC weather) — stay indoors on high-count days
- Wear wraparound sunglasses outdoors
- Shower and change clothes after being outdoors
- Apply petroleum jelly (Vaseline) around nostrils to trap pollen
- Keep car and house windows closed during peak pollen season
- Avoid drying clothes outside when pollen count is high
- Avoid cutting grass or being in freshly cut grass areas
Red Flags — Investigate Further
- Unilateral nasal symptoms — always investigate to exclude nasal polyp, foreign body or tumour
- Blood-stained nasal discharge — malignancy or granulomatous disease (GPA/Wegener's)
- Nasal polyps in a child — consider cystic fibrosis; refer for sweat test
- Anosmia not recovering after season — may indicate chronic rhinosinusitis or nasal polyps
- Hayfever symptoms out of season — reconsider; may be perennial rhinitis or other cause
- Worsening asthma during pollen season — review asthma management; consider step-up
- Suspected anaphylaxis to pollen (rare) — refer urgently to allergy clinic; prescribe adrenaline auto-injector
Clinical Features
- Nasal congestion, clear rhinorrhoea, sneezing, nasal itch
- Associated eye symptoms (allergic conjunctivitis) in 50%
- Seasonal (hay fever) — tree pollen (Mar-May), grass pollen (May-Jul), mould (Jul-Oct)
- Perennial — house dust mite, pet dander, mould
- Pale, boggy, bluish nasal mucosa on rhinoscopy
- Associated asthma, eczema, or food allergy in many patients
Immediate Management
- Allergen avoidance advice
- For mild/intermittent: non-sedating antihistamine — Cetirizine 10mg once daily, Loratadine 10mg once daily, or Fexofenadine 120mg once daily
Primary Care Management
- First-line: Intranasal corticosteroid — Mometasone furoate 100 micrograms (2 sprays) per nostril once daily, or Fluticasone propionate 100 micrograms (2 sprays) per nostril once daily; start 2 weeks before pollen season for hay fever
- Start 2 weeks before anticipated pollen season for hay fever
- For breakthrough symptoms: Cetirizine 10mg once daily, Loratadine 10mg once daily, or Fexofenadine 120mg once daily
- If poor response to monotherapy: Combined azelastine/fluticasone (Dymista) 1 spray per nostril twice daily
- Saline nasal irrigation as adjunct
- RAST/ELISA blood allergy testing or skin prick testing to identify allergens
- Advise on pollen avoidance strategies during high-count days
- If rhinitis coexists with asthma: Montelukast 10mg once daily at night (leukotriene receptor antagonist)
Specialist Referral Indications
- Inadequate response after 2-3 months of optimal pharmacotherapy
- Consideration for allergen immunotherapy (SCIT or SLIT)
- Associated nasal polyps or chronic rhinosinusitis
- Occupational rhinitis requiring investigation
- Severe uncontrolled symptoms affecting quality of life
Red Flags - Urgent Action Required
- Unilateral symptoms — exclude nasal polyp, foreign body or tumour
- Blood-stained discharge — malignancy or granulomatous disease
- Anosmia — may indicate nasal polyps or serious underlying pathology
- Facial pain with fever — complicated sinusitis or orbital cellulitis
- Nasal polyps in a child — consider cystic fibrosis (refer for sweat test)
Clinical Features
- Chronic cough — worse at night and on waking
- Sensation of mucus dripping down the back of the throat
- Frequent throat clearing
- Cobblestone appearance of posterior pharyngeal wall
- Associated with allergic rhinitis, sinusitis or vasomotor rhinitis
- Nasal discharge — clear (allergic/vasomotor) or purulent (infective)
- Hoarse voice — from mucus irritating the larynx
- Bad breath (halitosis)
- Sore throat from constant mucus contact
Immediate Management
- Identify and treat underlying cause
- Intranasal saline irrigation — first-line symptomatic relief
Primary Care Management
- First-line intranasal corticosteroid: Beclometasone dipropionate 100 micrograms (2 sprays) per nostril twice daily, or Mometasone furoate 100 micrograms (2 sprays) per nostril once daily — 4–6 week trial; if good response continue long-term
- Second-line (or adjunct if allergic component): Cetirizine 10mg once daily, or Loratadine 10mg once daily
- Avoid triggers — house dust mite reduction, pet allergen avoidance
- Humidifier at night if dryness is a contributing factor
- Avoid irritants: cigarette smoke, strong odours, chemical fumes
- Short-term decongestant spray if acute exacerbation — max 7 days
- Antibiotics only if bacterial sinusitis confirmed (purulent discharge >10 days)
- Review response at 6-8 weeks; step up if partial response
Specialist Referral Indications
- No response to 3 months of intranasal steroids
- Unilateral symptoms — exclude polyp, tumour, or foreign body
- Associated nasal polyps
- Suspected chronic rhinosinusitis requiring CT or endoscopy
Red Flags - Urgent Action Required
- Unilateral symptoms with blood-stained discharge — malignancy
- Haemoptysis — urgent investigation required
- Unexplained weight loss or night sweats — possible malignancy
- Persistent hoarseness >3 weeks — laryngeal pathology, 2WW referral
- Nasal obstruction with weight loss or cervical lymphadenopathy
- Facial pain or swelling — complicated sinusitis
Clinical Features
- Brief episodes of intense rotational vertigo (seconds to <1 minute)
- Triggered by head position change — rolling over in bed, looking up, bending forward
- No hearing loss or tinnitus
- Positive Dix-Hallpike test: rotatory upbeat nystagmus, 5-10s latency, fatigues on repetition
- Posterior semicircular canal most commonly affected (85-90%)
- May follow head trauma, viral illness, or prolonged bed rest
- Nausea is common; vomiting less so
- Episodes typically cluster then resolve spontaneously over weeks
Immediate Management
- Reassure — benign, self-limiting condition
- Perform Dix-Hallpike test to confirm diagnosis before commencing Epley
- Epley manoeuvre — 80% success rate after one treatment
- Demonstrate and teach home Brandt-Daroff exercises
Primary Care Management
- Perform Epley manoeuvre in clinic — can be repeated if needed
- Advise driving restriction until symptoms resolve
- Vestibular sedatives (prochlorperazine) not routinely recommended — may impair compensation
- If nausea/vomiting severe: Prochlorperazine 3–6mg buccal tablet (Buccastem) twice daily, or 5mg orally three times daily — use for maximum 2 weeks only to avoid impairing vestibular compensation
- Advise patient to avoid lying flat for 48 hours after Epley manoeuvre
- Review in 4 weeks — most resolve; teach Brandt-Daroff if persisting
Specialist Referral Indications
- Failed repeated Epley — consider horizontal canal BPPV variant
- Atypical nystagmus (direction-changing, no latency, no fatigue) — central cause
- Associated neurological symptoms — urgent
- Recurrent BPPV — consider vestibular rehabilitation
Red Flags - Urgent Action Required
- Nystagmus without latency, no fatigability — central cause (stroke, tumour)
- Associated diplopia, dysarthria, ataxia — posterior fossa stroke, emergency
- New onset headache with vertigo — subarachnoid haemorrhage
- Acute onset with unilateral hearing loss — labyrinthine infarction
- Prolonged vertigo (>1 minute continuous) — not typical BPPV, consider central cause
- Headache with new vertigo — possible subarachnoid haemorrhage
- Vertical nystagmus — always central in origin, urgent neurology referral
Clinical Features
- Perception of sound in one or both ears without external source
- Most commonly bilateral high-pitched ringing or buzzing
- Usually associated with sensorineural hearing loss
- Pulsatile tinnitus — synchronous with heartbeat; vascular cause until excluded
- Unilateral tinnitus with hearing loss — acoustic neuroma until excluded
- Common triggers: noise exposure, wax impaction, medication, stress, ototoxins
- Significant impact on sleep, concentration, and mental health
- Often worse in quiet environments — patients use background noise for relief
- Character varies: ringing, buzzing, hissing, whistling or clicking
Immediate Management
- Exclude reversible causes: wax, medication review, blood pressure
- Reassure: tinnitus rarely indicates serious pathology in most patients
Primary Care Management
- Otoscopy and check for wax — remove if present
- Review medications for ototoxins (NSAIDs, loop diuretics, aminoglycosides, quinine)
- Audiometry referral for full hearing assessment
- Advise on sleep hygiene and sound therapy — white noise apps, bedside sound machines, radio at low volume
- Tinnitus Retraining Therapy (TRT) or CBT for distressing tinnitus
- Hearing aids if associated hearing loss — may also reduce tinnitus perception
- Screen for anxiety and depression — comorbidity is common
- British Tinnitus Association resources: www.tinnitus.org.uk
Specialist Referral Indications
- Pulsatile tinnitus — urgent ENT for vascular imaging (MRI/MRA)
- Unilateral tinnitus — ENT for MRI IAM to exclude acoustic neuroma
- Associated sudden hearing loss — emergency ENT referral
- Objective tinnitus (audible to examiner) — urgent ENT
- Tinnitus not responding to primary care management at 3 months
Red Flags - Urgent Action Required
- Pulsatile tinnitus — vascular pathology (glomus tumour, AV malformation, carotid stenosis)
- Unilateral tinnitus with hearing loss — acoustic neuroma (MRI IAM)
- Associated neurological symptoms — intracranial pathology
- Objective tinnitus (heard by examiner) — vascular or palatal myoclonus
- Sudden onset tinnitus — may indicate sudden SNHL, treat as ENT emergency
Clinical Features
- Conductive or sensorineural — distinguish using Rinne and Weber tests
- Difficulty hearing conversation, especially in background noise
- Frequently asking others to repeat themselves
- TV or radio volume increased — often first noticed by family
- Social withdrawal, communication difficulties, low mood
- Gradual bilateral high-frequency loss = presbycusis (most common cause)
- Conductive loss: wax, OME, otosclerosis, perforation
- Sensorineural loss: noise-induced, ototoxicity, acoustic neuroma, sudden SNHL
- Unilateral SNHL with tinnitus — acoustic neuroma until proven otherwise
- Sudden SNHL (>30dB over 3 frequencies in <72h) = ENT emergency
Immediate Management
- If sudden SNHL: same-day ENT referral — if oral steroids started in primary care pending referral: Prednisolone 60mg once daily × 7 days then taper over 7 days (within 2 weeks of onset for benefit)
- Wax impaction: olive oil drops for 2 weeks then irrigation if needed
Primary Care Management
- Whisper test + otoscopy in all patients
- Rinne and Weber tuning fork tests to classify type
- Check for reversible causes: wax, OME, medication review (ototoxics)
- Refer to audiology for pure tone audiogram
- Adults >18 with bilateral SNHL: direct referral to NHS hearing aid services
- Review ototoxic medications (aminoglycosides, loop diuretics, cisplatin)
- Screen for depression — hearing loss significantly impacts mental health
- Consider urgent 2WW referral if unilateral hearing loss with suspicious associated symptoms
Specialist Referral Indications
- Sudden SNHL — same-day ENT (emergency)
- Unilateral SNHL — ENT for MRI IAM to exclude acoustic neuroma
- Conductive loss not explained by wax or OME
- Children with any hearing loss — urgent audiology
- Cochlear implant assessment if severe-to-profound bilateral SNHL
- Asymmetric hearing loss or associated tinnitus
Red Flags - Urgent Action Required
- Sudden onset hearing loss <72 hours — ENT emergency, same-day referral
- Unilateral hearing loss with tinnitus — acoustic neuroma (MRI IAM)
- Hearing loss with facial palsy or vertigo
- Blood-stained discharge with hearing loss — cholesteatoma or malignancy
- Pulsatile tinnitus with hearing loss — vascular pathology, urgent ENT + imaging
Conductive Hearing Loss
Common Causes:
- • Earwax impaction (most common)
- • Otitis media (acute/chronic)
- • Otosclerosis
- • Perforated tympanic membrane
- • Foreign body
- • Ossicular chain disruption
Test Results:
Weber: Lateralises to affected ear
Rinne: Bone conduction > Air conduction (negative)
Sensorineural Hearing Loss
Common Causes:
- • Age-related (presbycusis)
- • Noise-induced
- • Sudden sensorineural hearing loss
- • Ototoxic medications
- • Acoustic neuroma
- • Meniere's disease
Test Results:
Weber: Lateralises to unaffected ear
Rinne: Air conduction > Bone conduction (positive)
How to Perform Weber & Rinne Tests
Weber Test:
- 1. Strike 512Hz tuning fork
- 2. Place on centre of forehead/vertex
- 3. Ask "Where do you hear the sound?"
- 4. Normal: heard centrally
Rinne Test:
- 1. Strike 512Hz tuning fork
- 2. Place on mastoid process
- 3. When sound stops, move to ear canal
- 4. Ask if they can still hear it
- 5. Normal: AC > BC (positive Rinne)
Memory Aid
"Weber goes to the Worse ear in conductive loss, but to the Better ear in sensorineural loss"
Canalith Repositioning Procedure (CRP)
The Epley manoeuvre is the gold standard treatment for posterior canal BPPV, with an 80% success rate after a single treatment. This procedure repositions displaced otoconia (ear crystals) from the semicircular canals back to the utricle.
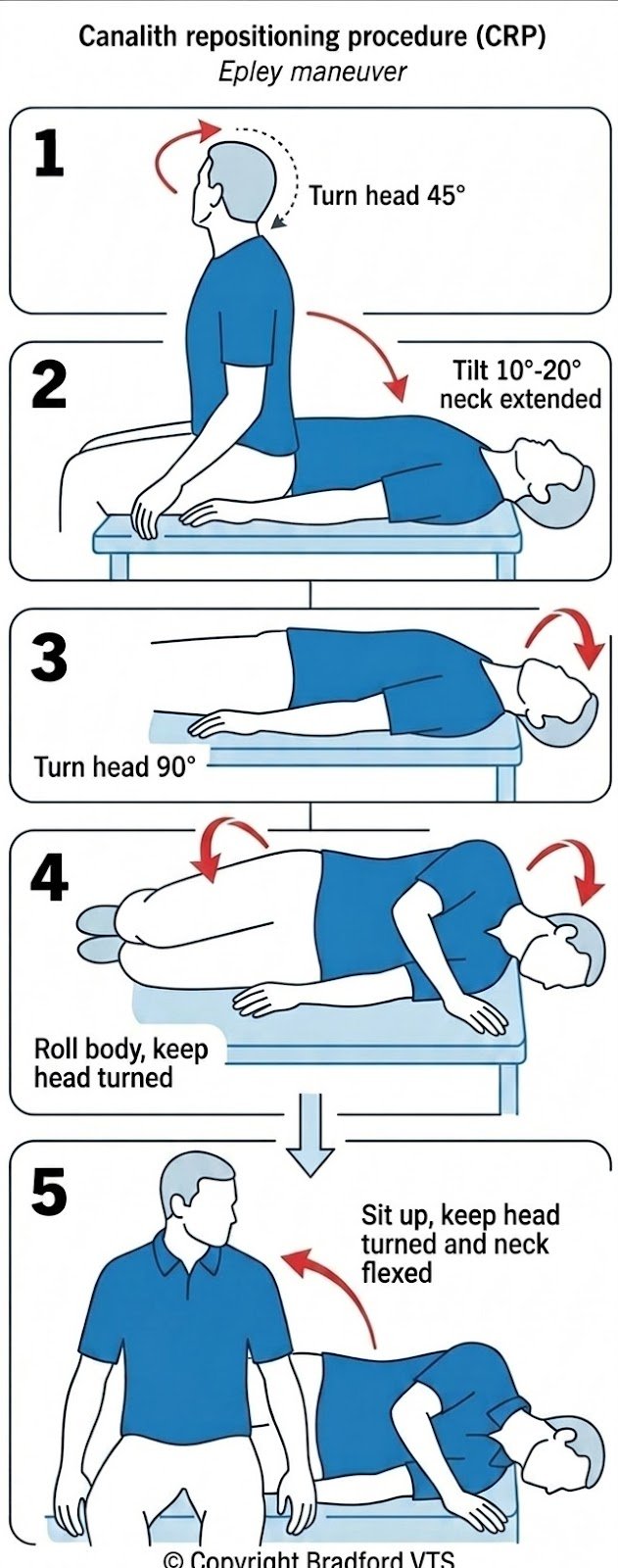
1 Starting Position
Sit with your head turned 45° toward the affected side. The patient should be sitting upright on the examination couch with legs extended.
2 Lie Back Position
Aided by your healthcare provider, lean back with one ear pointed toward the ground with your neck extended 10°-20°. The head should hang slightly off the edge of the couch. Wait 30 seconds or until vertigo subsides.
3 Turn Head to Opposite Side
Turn your head 90° toward the unaffected side. Keep your head in the extended position while turning. Wait another 30 seconds.
4 Roll to Side
Turn your head another 90° by rolling your body toward the unaffected side. You should now be lying on your side with your nose pointing downward at about 45°. Wait 30 seconds.
5 Return to Sitting
Sit up while keeping your head turned and neck flexed. Slowly return to an upright sitting position. The entire procedure takes about 2-3 minutes.
Clinical Tips
- • Each position should be held for 30 seconds
- • Vertigo and nystagmus are expected during the procedure
- • Can be repeated if first attempt unsuccessful
- • Success rate: 80% with single treatment
Post-Procedure Advice
- • Avoid lying flat for 48 hours after treatment
- • Sleep with head elevated (2 pillows)
- • Avoid rapid head movements for 24 hours
- • Symptoms may recur - teach patient home exercises
Significance
Potential for permanent hearing loss if not treated urgently
Action Required
Urgent ENT referral within 24 hours. Consider oral prednisolone.
Significance
Mastoiditis - complication of acute otitis media
Action Required
Same-day hospital admission for IV antibiotics and imaging
Significance
Epiglottitis - airway emergency
Action Required
Emergency admission. Do NOT examine throat. Call anaesthetics.
Significance
Peritonsillar abscess (quinsy)
Action Required
Same-day ENT referral for incision and drainage
Significance
Possible head and neck cancer
Action Required
2-week wait referral to ENT
Significance
Vascular cause (glomus tumour, AV malformation, carotid stenosis)
Action Required
Urgent ENT referral for imaging (MRI/MRA)
Significance
Acoustic neuroma (vestibular schwannoma)
Action Required
Routine ENT referral for MRI IAM
Significance
Risk of significant blood loss
Action Required
Emergency department for packing and coagulation management
Significance
Complication of otitis media or cholesteatoma
Action Required
Same-day ENT referral
Significance
Posterior circulation stroke
Action Required
Emergency stroke pathway activation
🎆 You've Got This!
ENT presentations can be challenging, but with systematic assessment, knowledge of red flags, and appropriate use of resources, you can provide excellent patient care. Remember: when in doubt, seek senior advice or specialist input.
🛡️ Safety Net
Always provide clear safety-netting advice and ensure patients know when to seek urgent review.
📊 Evidence-Based
Use NICE CKS and local guidelines to support your clinical decisions and antimicrobial stewardship.
📚 Continuous Learning
Reflect on cases, seek feedback, and use every patient encounter as a learning opportunity.