Training Diary: ST1 & ST2
in a GP Post
"Three years feels like forever — until you're in the middle of it. Here's your map, your compass, and your survival guide."
📥 Downloads
path: TUTORIAL SUGGESTIONS FOR ANY STAGE OF GP
- 10 golden rules for general practice.docx
- being therapeutic - laughter as medical therapy.ppt
- being therapeutic - when listening is the therapy - the patients lament - hidden key to effective listening.pdf
- being therapeutic - when listening is the therapy - the patients lament - turning moaning into therapy.pdf
- clinical - clinical examination - is it really necessary (TEACHING RESOURCE).ppt
- clinical - emergencies assessment questionnaire EmAQ.doc
- clinical - spotting the sick child in 3 minutes.doc
- clinical examination as a therapeutic examination.docx
- decisions - cognitive biases.ppt
- decisions - complexity and how doctors think.pdf
- decisions - fast and slow thinking systems.docx
- decisions - how doctors solve problems.docx
- decisions - pattern recognition in the consultation.doc
- decisions - perceptual capacity and the gp.docx
- decisions - prioritising making decisions and managing your time.docx
- decisions - RAPRIOP management options.docx
- decisions - when no diagnostic label is applied.docx
- information technology - using the computer in the consultation.docx
- learning and develoment - core values - what makes you tick.docx
- learning and development - 2 minutes on Educational Change.docx
- learning and development - 2 minutes on Motivation for Learning.docx
- learning and development - feedback - basic principles of.docx
- learning and development - feedback - receiving.docx
- learning and development - keeping clinically up to date - good and bad doctors.doc
- learning and development - learn every day in every way.pdf
- learning and development - motivating values.docx
- learning and development - novels about general practice.docx
- learning and development - personal values - what makes you tick.docx
- learning and development - self actualisation level.docx
- learning and development - self fulfillment - self actualisation index.docx
- learning and development - wheel of life - hows your life currently going.docx
- learning and development - winners and losers - what are you.doc
- mrcgp professional capabilities.docx
- person centred medicine - 5 things all patients want to HAPPEN.ppt
- person centred medicine - 5 things all patients want to KNOW.ppt
- person centred medicine - 5 things all patients want.docx
- person centred medicine - a story (after Candide) - individual vs population medicine.docx
- person centred medicine - being therapeutic by encouraging the narrative thread.docx
- person centred medicine - disease vs illness.docx
- person centred medicine - disease vs illness.ppt
- person centred medicine - how to do it.docx
- person centred medicine - the health belief model.docx
- person centred medicine - triangular thinking in general practice.docx
- person centred medicine - why patients go to the doctor.docx
- politics - how tainted is medicine - the big pharma.doc
- politics - left vs right wing - what does it all mean.doc
- politics - the NHS race.pps
- prescribing - 10 tips for safer prescribing.pdf
- prescribing - high risk medications for causing errors.pdf
- probophilia - quality versus quantity - are we counting the wrong things.pdf
- what makes a good gp - braunack.pdf
- what makes a good gp - leck and leck.pdf
- what makes a good gp - perceptual capacity.doc
- whats a good doctor and how do you make one by rizo et al.docx
- when no diagnostic label is applied by jones et al.docx
🌐 Web Resources
RCGP WPBA Mandatory Evidence Sheet
The definitive table of exactly how many assessments you need, per year and per placement.
Visit RCGP WPBARCGP Professional Capabilities Framework
The 13 capabilities that underpin every assessment, log entry, and ARCP judgement you will face.
View CapabilitiesFourteenFish ePortfolio
Your ePortfolio home — log entries, assessments, ESRs, CSRs, and ARCP evidence all live here.
Log InProfessional Capability Cheat Sheet
Bradford VTS's own plain-English summary of all 13 capabilities — far more readable than the original.
Read ItRam's Easy Peasy Learning Log Guide
The single most practical guide to writing ePortfolio log entries that actually impress ARCP panels.
Read GuideLearning Logs & Reflection Pages
Understanding reflection properly transforms your log entries from tick-box waffle into real learning evidence.
ExploreCBD Resources Page
Everything you need to do a Case-Based Discussion well — including hints trainers won't always volunteer.
View CBDsCOT Resources Page
How to do a Consultation Observation Tool properly — including recording, reviewing, and discussing.
View COTsEducational Supervision Pages
How to prepare for your ESR — including the evidence rating scales, action points, and PDPs.
Prepare NowQuality Improvement Projects
Practical QI guidance — including examples, theory, and templates. Do your QIA in ST1, not ST3.
QI ResourcesUUC & Out-of-Hours Page
Everything about Urgent Unscheduled Care — how to record sessions, reflect on capabilities, and stay safe.
UUC GuideHow to Study Effectively
The research on learning methods — some of what you think works, doesn't. ST1 is the ideal time to find out.
Study SmartPersonal Development Plans (PDPs)
How to write SMART PDPs that are genuinely useful — not just ticked boxes for your supervisor's peace of mind.
PDP GuideTypingClub.com
If your typing speed is below GP-survival level, start now. Everything in modern general practice is electronic.
Practice TypingARCP Panels — What To Know
Demystifying the Annual Review of Competence Progression — what panels look for and how to prepare your evidence.
ARCP Guide⚡ Quick Summary
Rushing to a tutorial? Preparing for your ESR? Start here. This box is your entire ST1/ST2 GP post in a nutshell.
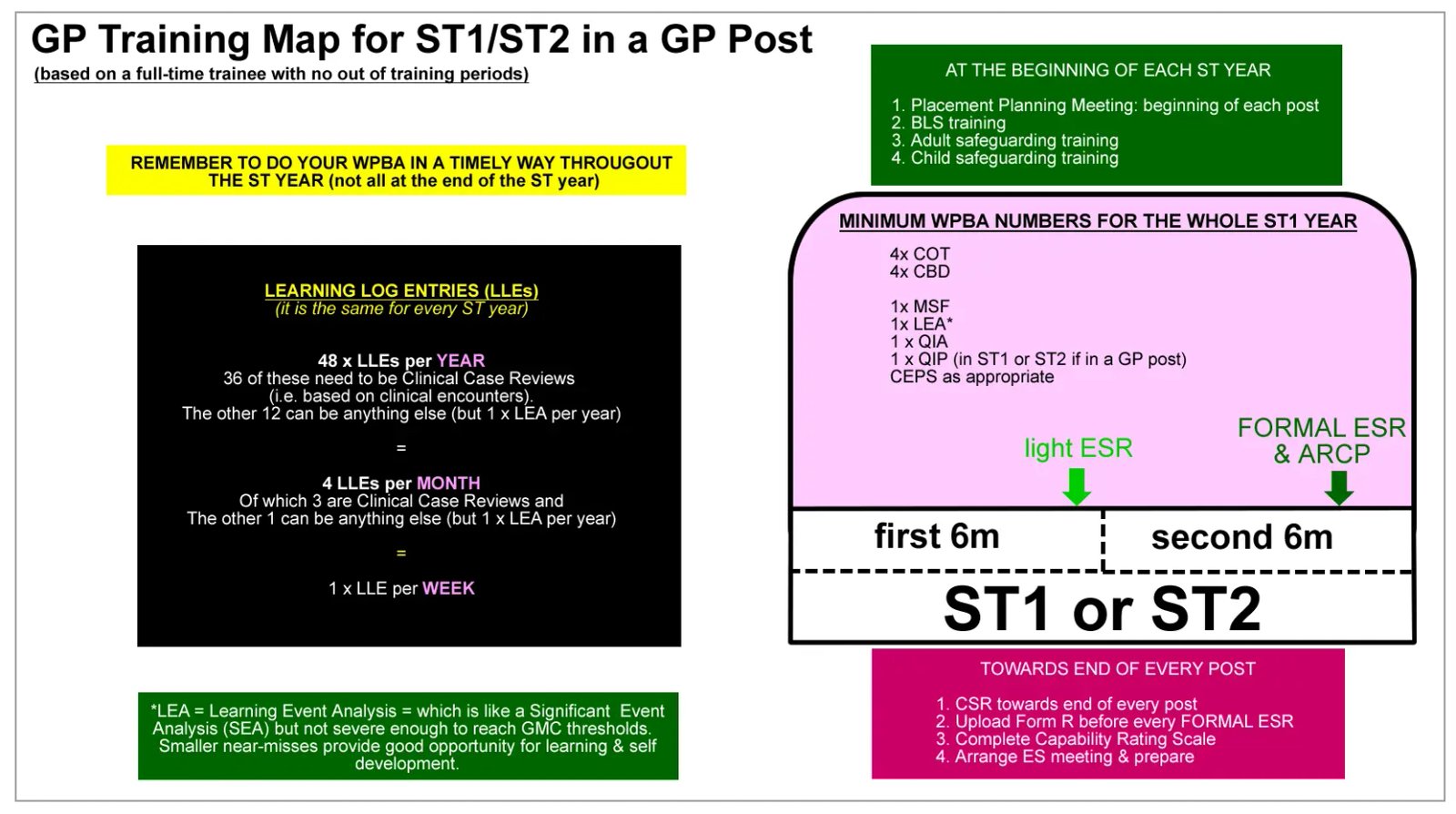
The ST1 & ST2 GP post training map — your visual overview of the whole placement
ST1 & ST2 in GP — If You Only Read One Thing
Your Training Diary at a Glance
🎯 The Big Picture
- ST1/ST2 GP posts develop you across 4 pillars: Relationships, Decision-Making, Management, and Professionalism
- Everything is underpinned by the 13 Professional Capabilities — understand these early
- Your ePortfolio is your evidence to the world — it is how ARCP panels know you exist
- Aim for 1 log entry per week — that's 4 per month, 3 on clinical cases
- Do your WPBAs regularly — never leave them all to the last month
- QI project: start in ST1. Do not leave this until ST3
- OOH: roughly one session per month once you are in a GP post
📋 Key Numbers (WPBA)
- CBDs: minimum 4 per training year (ST1 & ST2)
- COTs: 2 per GP placement (COTs = GP posts only)
- MiniCEX: 2 per hospital placement
- COT + MiniCEX combined minimum: 4 per training year
- MSF: 1 full cycle in ST1 (and again in ST3)
- PSQ: required in GP placements
- CEPS: relevant to post in both ST1 and ST2
- Always verify latest numbers at rcgp.org.uk/mrcgp-exams/wpba
🎯 Why This Matters in GP Training
ST1 and ST2 feel like the "early" years — but the habits, systems, and mindset you build now follow you all the way to CCT and beyond.
Foundations Are Set Here
Your approach to consultations, reflection, and self-management in ST1 becomes your default mode. Good habits established early are hard to lose.
Your ePortfolio Starts Now
ARCP panels use your ePortfolio to make progression decisions. Gaps, thin evidence, or late entries in ST1 create problems that compound in later years.
ST1 Is Your Breathing Space
ST1 is the least pressured year. You have time to learn properly. ST3 has the MRCGP, a mountain of assessments, and very little time. Use ST1 wisely.
GP Is Very Different to Hospital
Time pressure, undifferentiated presentations, lone decision-making, and holistic patient management — none of these fully prepared you in FY training.
NHS Context Needs Learning
PCNs, QOF, LMCs, referral pathways, patient access — all of this is unique to UK general practice. Understanding the system is part of the job.
Relationships Define GP
The therapeutic relationship with patients and working relationships with colleagues are the engine of general practice. They are assessed formally and informally from day one.
📘 Training Structure & the RCGP 2025 Curriculum
How your working week is structured, how your appointment times should progress, and what changed in the August 2025 curriculum update — all in one place.
🗓 Your GP Post Working Week
A standard full-time ST1/ST2 GP placement week is structured as:
| Component | Sessions per week |
|---|---|
| Clinical sessions | 7 |
| Educational sessions | Up to 3 (HDR, tutorials, self-directed study) |
⏱ Appointment Time Progression
Your consultation slot length should evolve with your confidence:
| Phase of Placement | Appointment Length |
|---|---|
| First 4 weeks | 30 minutes |
| Months 2–4 | 20 minutes |
| Month 5 onwards | 15 minutes |
📘
RCGP 2025 Curriculum Update — What Changed?
An evolution, not a revolution. Assessment formats unchanged. Key structural changes that are exam-relevant.
▾
RCGP 2025 Curriculum Update — What Changed?
An evolution, not a revolution. Assessment formats unchanged. Key structural changes that are exam-relevant.
🆕 New Clinical Topic Guides
- Learning Disability — now a standalone guide
- Maternity & Reproductive Health — moved from Life Stages into the Clinical Topic Guide list
- Neurodevelopmental conditions & neurodiversity (autism, ADHD) — split from previous combined guide
✏️ Renamed Guides (Contemporary Terminology)
- Allergy and Immunology → Allergy & clinical immunology
- Gynaecology and Breast → Gynaecology & breast health
- Kidney and Urology → Renal & urology
- Infectious Disease and Travel Health → Infectious diseases & travel health
🌍 New Content Emphases (embedded throughout)
- COVID-19 long-term impacts on practice
- Climate change and health (planetary health)
- Digital consultations and remote care
- Personalised care perspectives
- Social determinants of health
📋 Overall Topic Guide Structure (2025)
- Professional: 6 guides (consulting, EDI, evidence, quality & safety, leadership, population & planetary health)
- Life Stages: 4 guides (children & YP, LTCs, older adults, end of life)
- Clinical: 22 guides (including the 3 new/moved ones above)
📋 WPBA Quick Reference
At a glance: which assessments, how many, and in which setting. Verify the latest numbers at rcgp.org.uk/mrcgp-exams/wpba — this is your responsibility, not your trainer's.
| Assessment | Where Done | ST1 Minimum | ST2 Minimum | Notes |
|---|---|---|---|---|
| CBD Case-Based Discussion |
GP post or hospital | 4 per year | 4 per year | 2 per 6-month placement; you choose the cases |
| COT Consultation Observation Tool |
GP post only | 2 per GP placement (4 combined COT+MiniCEX per year) |
Includes audio COT, face-to-face, and virtual | |
| MiniCEX Mini Clinical Evaluation Exercise |
Hospital only | 2 per hospital placement (4 combined COT+MiniCEX per year) |
Assessed by consultant or registrar ST4+ | |
| MSF Multi-Source Feedback |
Any post | 1 full cycle in ST1 | Not required (ST1 & ST3 only) | Min. 10 respondents; mix of clinical and non-clinical |
| PSQ Patient Satisfaction Questionnaire |
GP post only | As directed by deanery | Min. 40 patient responses; completed in GP posts | |
| CEPS Clinical Examination & Procedural Skills |
Any post | Relevant to post | Must show range; intimate examinations by end of ST3 | |
| Learning Logs (CCRs) | Any post | 1 per week recommended 3 per month as clinical case reviews |
Must address all 13 capabilities; must show reflection + learning | |
| QIA/QIP | GP post only | 1 per training year | 1 per training year | QIP (Quality Improvement Project) counts if done in GP post |
| CSR Clinical Supervisor's Review |
Every post | 1 per post | Your trainer must complete this; chase them! | |
| ESR Educational Supervisor's Review |
Every post | Every 6 months | Preparation is your responsibility — allow 2–3 hours | |
| PDP Personal Development Plan |
Every post | 3–5 SMART goals per post | Set at start of post; review at ESR | |
| Form R | — | Annually | Must be uploaded to portfolio; TOOT days must match | |
| BLS / Safeguarding | Courses | Each training year | Face-to-face with active participation; add to compliance passport | |
🏛 The Four Pillars of Your GP Post
Every part of your job as a GP — clinical and non-clinical — sits within these four domains. They are the framework your Placement Planning Meeting uses. Understand them before you sit down with your trainer.
Pillar 1 — Relationship Skills
Communication, consultation craft, rapport, and working relationships with colleagues
▾
Pillar 1 — Relationship Skills
Communication, consultation craft, rapport, and working relationships with colleagues
By End of This Placement, the Trainee Will…
- Be building strong rapport with patients across face-to-face and telephone consultations
- Be moving from 30-minute to 15-minute consultations on average
- Show good working relationships with all staff — not just doctors
- Demonstrate respect for differing opinions in practice meetings
📚 How to Develop It
- Read a communication skills book (The Inner Consultation, The Naked Consultation)
- Record and review your own consultations
- Practise telephone consultations actively
- Engage genuinely with all colleagues — admin, nursing, allied health
- Tutorials and professional conversations with your trainer
📊 How It Is Measured
- COTs — especially history-taking, explanation, and patient involvement
- MSF — comments from all staff, not just clinical colleagues
- Log entries — reflecting on specific micro-skills (ICE, PSO, signposting, explanations)
- Practice meeting behaviour — does the trainee contribute, or just sit quietly?
- Thank-you cards and patient feedback
Pillar 2 — Decision-Making Skills
Diagnosis, clinical reasoning, management plans, knowing your limits
▾
Pillar 2 — Decision-Making Skills
Diagnosis, clinical reasoning, management plans, knowing your limits
By End of This Placement, the Trainee Will…
- Handle most consultations adequately, seeking advice less and less as the post progresses
- Make reasonable working diagnoses and think about differential diagnoses
- Know where to find information quickly when they don't know something
- Know their clinical limits — and know when they are too unwell to practise safely
- Handle results, letters, and home visits safely (all debriefed at ST1/ST2 level)
📚 How to Develop It
- Face-to-face and telephone consultations — with debrief every time at this stage
- Build your personal "where to look" flow diagram — NICE CKS? GPNotebook? BNF?
- Tutorials on clinical topics with your trainer
- Reflect on clinical decision-making in your log entries
- HDR sessions and workshop attendance
📊 How It Is Measured
- Daily debriefs — gradual decrease in advice-seeking over the post
- CBDs — data gathering, diagnosis, clinical management
- COTs — appropriate working diagnosis and management plan
- MSF — colleagues say clinical acumen is sound
- Log entries — demonstrate decision-making thinking
Pillar 3 — Management Skills
Time management, admin systems, workload prioritisation, self-care, resilience
▾
Pillar 3 — Management Skills
Time management, admin systems, workload prioritisation, self-care, resilience
By End of This Placement, the Trainee Will…
- Understand the systems that make a GP practice function
- Prioritise their daily workload — clinical and educational
- Complete admin on time: prescriptions, referrals, results, letters
- Engage actively with their own learning and development
- Recognise when they are stressed or too unwell to perform safely
📚 How to Develop It
- Develop your own daily routine — tasks, letters, results, email, pigeon hole
- Engage with clinical IT systems: EMIS, SystmOne, ICE, pathlinks, referrals
- Attend BLS, safeguarding, and mandatory courses early
- Discussions at HDR about personal management and resilience
- Consider self-management courses if resilience is a concern
📊 How It Is Measured
- Observed surgeries — effective computer use, referral systems
- MSF — no concerns about paperwork or missed tasks
- Educational engagement — prepares for tutorials, HDR, presentations
- CBDs — progressing in OML, managing complexity, working with colleagues
- ePortfolio — timely entries, reflects on work-life balance
Pillar 4 — Professionalism
Respect for patients, colleagues, the record, and the training process itself
▾
Pillar 4 — Professionalism
Respect for patients, colleagues, the record, and the training process itself
By End of This Placement, the Trainee Will…
- Demonstrate genuine respect for patients — as fellow human beings, not cases
- Show genuine respect for contractual responsibilities
- Engage constructively with feedback — including critical feedback
- Treat the ePortfolio, WPBAs, and training requirements with genuine respect
- Begin to understand the need to rationalise care and protect NHS resources
🔴 Critical Warning — Medical Records
- All medical systems have a full audit trail — word by word, time-stamped
- Every change you make to a record is permanently logged
- Never alter records retrospectively — instead, add a new dated note
- This is a legal and regulatory issue, not just an etiquette one
📊 How It Is Measured
- MSF — professionalism, attitude to work, going the extra mile
- COTs — shows respect for the assessment; selects own consultations thoughtfully
- CBDs — preparation shows care and respect for the process
- Thank-you cards and patient comments
- Absence patterns — both too much and too little can indicate self-management issues
🗓 The Three Training Phases
Your 6-month GP post is divided into three actionable phases. Each phase has clear priorities. Click each phase to see exactly what to focus on and why.
🌱
Phase 1 — The First 4 Weeks
Orientation, orientation, orientation. Get your systems right before anything else.
▾
Phase 1 — The First 4 Weeks
Orientation, orientation, orientation. Get your systems right before anything else.
Understand the 13 Professional Capabilities
Everything you are assessed on — every log entry, every WPBA, every ARCP — maps to these 13 capabilities. Getting a real grip on them now pays dividends for three years.
Professional Capabilities & Cheat SheetUnderstand Learning Log Entries — Before Writing Any
Most trainees dive in and write pages of description. The educational point is reflection and learning — not narration. Read Ram's guide before you write your first entry.
Ram's Easy Peasy Log GuideUnderstand Reflection — the Engine of Log Entries
Learning cannot happen without reflection. Reading about reflection before writing logs transforms the quality of every entry you produce. Worth an hour of your time.
Reflection PagesAttend Your Scheme Induction — and Attend It Early
Your TPD's scheme induction gives you the whole picture of GP training in one go. It is not optional. Find the dates before your post starts, and book study leave immediately.
Scheme Induction ResourcesSit In With Different Staff Members
Who does what? What can a pharmacist prescribe? What does the district nurse do differently from the practice nurse? What happens to a prescription after you sign it? Find out now.
Task-Sheets for Sitting InPlay With the Medical Computer System
EMIS, SystmOne, or Vision — find the test patient and explore without consequence. Ask your Practice Manager to set up a session. Also explore ARDENS and any add-on systems.
Log in to FourteenFishFamiliarise Yourself With Your ePortfolio
Log into FourteenFish 3–4 times a week for the first two weeks — just to click around and get a feel for it. The last thing you want is a technical barrier when you have something meaningful to write.
FourteenFish LoginDefine Your Daily Work Routine
Without a system for admin, you will miss things. Ask your trainer what their own post-surgery routine looks like. Then adapt it: clinical tasks → letters → results → pigeon hole → email.
Plan Your English — If You Need To
If you qualified outside the UK and want to improve your English for the SCA: start now, not in ST3. TV series, audiobooks, English conversation outside work — build a weekly plan and stick to it.
📍 First 4 Weeks Survival Checklist
👥 People to Meet
- ✓ Your GP Trainer
- ✓ Practice Manager
- ✓ Reception lead
- ✓ Secretarial / referral team
- ✓ Prescribing lead / pharmacist
- ✓ Nursing team
- ✓ Duty doctor / on-call system
- ✓ HCA and phlebotomist
⚙️ Systems to Learn
- ✓ How blood results are processed
- ✓ How letters and Docman work
- ✓ Referral pathways (including 2WW)
- ✓ Prescribing system and repeat rules
- ✓ Task workflow (who does what)
- ✓ Safeguarding alert process
- ✓ Home visit booking system
- ✓ Who to call if a patient deteriorates same day
📝 Things to Do
- ✓ Sit in clinics across all staff types
- ✓ Start supervised consultations
- ✓ Debrief every surgery session
- ✓ Log in to FourteenFish — explore before pressure hits
- ✓ Find local referral guide and keep it handy
- ✓ Start a "practice systems notebook" — learn once, don't repeat errors
- ✓ Agree your Placement Planning meeting date
🌿
Phase 2 — Months 1 to 3
Building momentum: ePortfolio habits, WPBAs, communication skills, and how to study.
▾
Phase 2 — Months 1 to 3
Building momentum: ePortfolio habits, WPBAs, communication skills, and how to study.
Book Your Courses With Plenty of Notice
At least 6 weeks' notice for any course — GP practices and hospitals cannot release you at the drop of a hat. Priority courses: BLS, safeguarding (adult & child), GP update courses, family planning, OOH preparation.
Start Reading a Consultation Skills Book
Pick one and read it properly. Good communication skills make your consultations faster, safer, and more enjoyable — and they are directly assessed in COTs and the SCA exam. Do not leave this until ST3.
Communication Skills DatabaseUnderstand WPBA — Then Do Your First COT & CBD
Read about all WPBA tools before you do your first one. Understanding the purpose makes the assessment more useful and means you approach it with the right mindset, not just to tick a box.
Intro to WPBATarget 1 Log Entry Per Week
By now, aim for roughly one per week — 4 per month. Three should be Clinical Case Reviews about real patients you have personally seen. The fourth can be anything: an HDR session, a teaching point, a significant event reflection.
Learning Logs & ReflectionLearn How to Study Effectively
Most of us were never taught effective study techniques. Some of what we think works is actually inefficient. ST1 — the easiest year — is the ideal time to read the evidence and change your habits.
How to StudyConsider Running an HDR Teaching Session
Teaching others is one of the most powerful ways to consolidate your own learning. If you are asked to present at HDR, learn some basic teaching theory first — it takes the experience from uncomfortable to genuinely educational.
Teaching for BeginnersExplore Bradford VTS Regularly
Over 2000 resources covering everything from clinical pages to communication skills to QI. You do not need to read everything now — dip in and out over three years. But visiting regularly keeps your learning refreshed and prevents the "I wish I'd known about this sooner" feeling.
🌳
Phase 3 — The Last 3 Months
Demonstrating progress: ePortfolio review, QI project, PDPs, ESR & CSR preparation.
▾
Phase 3 — The Last 3 Months
Demonstrating progress: ePortfolio review, QI project, PDPs, ESR & CSR preparation.
Review Your ePortfolio — Honestly
If it is going badly, work out why and discuss it with your trainer. Thin entries, missing capabilities, or poor reflection are fixable now — not after the ARCP. Are all 13 capabilities covered? Are your entries showing genuine evidence of learning?
Evidence for Capability Rating ScalesComplete Your Second COT & CBD
By the end of ST1, aim for a minimum of 4 CBDs and 4 COTs/MiniCEX for the year. That means 2 of each in this placement and 2 in the next. Do not leave both to the final two weeks — it shows poor organisation and the quality suffers.
CBD PageDo Your QI Project — Now, Not Later
One QIA/QIP is required per training year. ST1 is the right time — the easiest year, when you have time to do it properly. It must be done in a GP post. In ST3, you will have the MRCGP exams on top of everything else. Do not leave this.
QI Theory & ProjectsReview & Complete Your PDPs
Were your PDP goals SMART? Are you on track to achieve them? Prepare to discuss progress at your ESR. Also start drafting PDPs for your next post — your Educational Supervisor will expect them.
PDP ResourcesEngage With UUC / Out-of-Hours
If you are in a GP post, you should be doing roughly one OOH session per month — mostly observational at this stage. Tell your practice you need time off to not exceed the 40-hour working week limit. Write up each session in your ePortfolio.
UUC & OOH PagePrepare Your ESR & Ask for Your CSR
Allow 2–3 hours to prepare your ESR properly. Focus on: (1) evidence for capability self-rating scales, (2) formulating action points, (3) PDPs. Also ask your trainer explicitly to complete your Clinical Supervisor's Review — it will not happen automatically.
Educational Supervision Pages🏥 Maximising GP Learning in Hospital Posts
Every hospital post is a GP post in disguise — if you look at it the right way. The question to ask after every ward round: "What would this patient have looked like in a GP consultation six months ago?"
🌐 Universal Principles — Apply in Every Post
Placement Planning Meeting
Within 3 weeks of starting. Bring a written PDP — this signals motivation and usually results in better teaching.
Ask: "What in GP?"
After every ward round: what brought them to their GP first? What were the early signs? Could it have been managed in primary care?
Map to RCGP Topic Guide
Most cases map to one of 22 clinical topic guides. Use this to drive log entries and ensure broad ARCP coverage.
Document within 48 hours
Clinical detail fades fast on busy hospital posts. Write case reviews the same day or next day — not at the weekend.
Cover all 12 Clinical Experience Groups
ARCP panels want breadth across all groups. Check your coverage map in FourteenFish regularly.
Click a specialty to see the key GP learning points, AKT tips, and ePortfolio strategy:
🏨
Acute Medicine / AMU
Frailty, polypharmacy, sepsis, acute HF, COPD, PE, ACS, delirium
▾
Acute Medicine / AMU
Frailty, polypharmacy, sepsis, acute HF, COPD, PE, ACS, delirium
🎯 Key GP Learning Points
- Frailty & CGA — Comprehensive Geriatric Assessment maps directly to GP management of frailty, falls, and multimorbidity
- Polypharmacy & deprescribing — the AMU patient on 10 medications is your future GP patient
- Discharge planning — what was not sorted? Who does follow-up? This creates GP workload — understand it
- Common acute presentations — acute HF, COPD exacerbation, PE, ACS, delirium, diabetic emergencies
🔥 AKT Tips from AMU
- qSOFA criteria for sepsis: Respiratory rate ≥22, altered mentation, systolic BP ≤100 — know all three for AKT
- NEWS2 scores — understand scoring and clinical triggers
- Sepsis can be occult — normal obs do not exclude it
- Delirium in elderly = look for precipitants (infection, medication, constipation, pain)
🧠
Psychiatry
Risk assessment, MSE, psychiatric medications, MHA sections, community pathways
▾
Psychiatry
Risk assessment, MSE, psychiatric medications, MHA sections, community pathways
🎯 Six Key GP Learning Areas
- Risk assessment — Columbia Severity Rating Scale; document protective factors as well as risks
- Mental State Examination (MSE) — appearance, behaviour, speech, mood, affect, thought form/content, perception, cognition, insight
- Psychiatric medication — SSRIs, SNRIs, mirtazapine, antipsychotics (olanzapine, risperidone, quetiapine, aripiprazole), mood stabilisers, monitoring requirements
- Community psychiatry — CMHT, CRHTT, IAPT, AMHP, Section 136
📋 Mental Health Act — Quick Reference
- Section 2 — Assessment, up to 28 days
- Section 3 — Treatment, up to 6 months
- Section 4 — Emergency, up to 72 hours
- Section 5(2) — Doctor's holding power
- Section 5(4) — Nurse's holding power
- Section 136 — Police power to remove to place of safety
🔥 AKT Tips from Psychiatry
👶
Paediatrics
Traffic light system, development, safeguarding, immunisations, common presentations
▾
Paediatrics
Traffic light system, development, safeguarding, immunisations, common presentations
🎯 Key GP Learning Points
- Traffic light system — NICE fever in under-5s: Green / Amber / Red — practise applying it on every child
- Child development — normal and abnormal milestones; use developmental history in every child consultation
- Safeguarding — local procedures, referral pathways, child protection register; non-urgent vs urgent referrals
- Immunisation schedule — indications, contraindications, common side effects, PGDs
🩺 Common GP Paediatric Presentations
- Viral illness and fever management
- Ear pain and otitis media
- Wheeze and asthma
- Eczema management
- Behavioural and developmental concerns
- Enuresis and encopresis
- Growth concerns and faltering growth
🤰
Obstetrics & Gynaecology
Antenatal care, ectopic pregnancy, contraception, HRT, miscarriage, cervical screening
▾
Obstetrics & Gynaecology
Antenatal care, ectopic pregnancy, contraception, HRT, miscarriage, cervical screening
📅 Antenatal Care Structure
- Booking: 8–10 weeks
- 12w: USS + bloods (Down's screening)
- 20w: Anomaly scan
- 28w: Repeat bloods (FBC, antibodies)
- 36w: Presentation check
- 41w: Post-dates assessment + IOL discussion
🚨 High-Yield GP O&G Points
- Ectopic pregnancy: Any woman of reproductive age with amenorrhoea + abdominal pain → pregnancy test. If positive and in pain → urgent referral
- HRT (NICE 2024): Offer for menopausal symptoms; low risk in healthy women <60 within 10 years of menopause; transdermal preferred for VTE risk
- Miscarriage: Expectant / medical (mifepristone + misoprostol) / surgical; anti-D for rhesus negative women
- Cervical screening: Starts age 25 in England; 3-yearly 25–49; 5-yearly 50–64
🚑
Accident & Emergency
ABCDE approach, high-acuity presentations, practical skills, what returns to GP
▾
Accident & Emergency
ABCDE approach, high-acuity presentations, practical skills, what returns to GP
🎯 Key GP Learning Points
- ABCDE approach — systematic and reproducible; practise until automatic
- High-acuity early recognition: Sepsis, PE, MI, stroke, DKA, hypoglycaemia
- Practical skills: IV access, ABGs, ECG interpretation, suturing, plastering, FAST scan observation — grab opportunities
- What returns to GP: Every discharge generates a potential follow-up need — understanding A&E helps you triage in primary care
🔥 AKT Tips from A&E
- PE: Wells score → D-dimer if low probability; CTPA if raised or high probability
- STEMI vs NSTEMI: STEMI = ST elevation or new LBBB → primary PCI; NSTEMI = troponin rise without ST elevation
- DKA criteria: glucose >11, pH <7.3, bicarbonate <15, ketones >3 — know all four
- Hypoglycaemia in conscious patient: 15–20g fast-acting glucose; recheck in 15 mins
📁 ePortfolio Strategy for Hospital Posts
📋 Minimum Requirements per Year
- ✓ 36 Clinical Case Reviews (3 per month)
- ✓ Placement Planning Meeting within 3 weeks of each post
- ✓ Clinical Supervisor Report at end of each post
- ✓ MSF — required twice in ST1; complete early in the year
- ✓ Learning Event Analysis (LEA) and Significant Event Analysis (SEA)
✍️ Making Hospital Reflections Count
- ✓ Reflect on your decision-making — not the consultant's
- ✓ If you disagreed with a management decision — reflect on it; this shows independent thinking
- ✓ Tag at least 2 curriculum capabilities per entry
- ✓ Link each case to an RCGP Topic Guide knowledge section
- ✓ Quantify learning: "Before: didn't know X. Now: know Y. Next time: will do Z."
🩺 GP Action Framework
This is the practical heart of your early GP placement. What does "safe, good enough for ST1" actually look like — and how do you operate safely every single day? Here is the framework that experienced trainers actually use to judge early performance.
✅ What Your Trainer Really Wants to See by End of Placement
You do not need to be polished. You need to be safe, organised, coachable, and progressively more independent.
Usually identifies the main presenting problem without needing prompting
Spots obvious red flags and acts on them — does not need the trainer to catch them
Makes a sensible working diagnosis — not necessarily correct every time, but reasonable and explained
Knows when to ask for help and asks before the situation becomes unsafe
Documents clearly enough for the next clinician — not a wall of text, not a one-liner
Converts debrief feedback into changed behaviour next time — not repeating the same mistakes
Manages basic admin safely — results actioned, letters processed, tasks completed on time
Knows when the consultation is drifting — and gently redirects it rather than losing the thread
🔄 Your Per-Patient Consultation Routine
Ask yourself these six questions for every patient — before you close the record:
| # | Self-Check Question |
|---|---|
| 1 | What is the main issue today? |
| 2 | Is there anything dangerous here I must not miss? |
| 3 | What is my working diagnosis? |
| 4 | What is my immediate plan — and can the patient actually follow it? |
| 5 | What follow-up or safety-net have I arranged? |
| 6 | Do I need to discuss this now with my supervisor? |
📋 Your Admin Safety Routine
For every result, letter, or task — ask these six questions. The real risk in admin is not diagnostic; it is administrative drift.
| # | Question to Ask |
|---|---|
| 1 | What does this show? What is the abnormality? |
| 2 | Does it need action — and how urgent is that action? |
| 3 | Who is responsible for taking the action? |
| 4 | Has the patient been informed? |
| 5 | How will continuity happen — who picks this up next? |
| 6 | What is the fail-safe if the next step does not happen? |
🙋 How to Ask for Help Well — Structured Escalation
Asking for help is not a sign of failure — it is a sign of professionalism. But how you ask for help matters. Use this structure every time you interrupt your trainer or duty doctor:
| Element | What to say | Example |
|---|---|---|
| Main concern | "My main concern is…" | "My main concern is that this could be a PE." |
| Key positives | "The key features pointing that way are…" | "He has pleuritic chest pain, a recent long-haul flight, and his O₂ is 94%." |
| Key negatives | "I've checked for X and it's reassuring that…" | "There's no leg swelling, no haemoptysis, and his HR is normal." |
| Working diagnosis | "My working diagnosis is…" | "I think this most likely is a PE but I'm not confident." |
| What you need | "I need your help with…" | "I need help with the next step — is this a 999 call or urgent referral?" |
"I'd like to discuss this with my supervising GP before finalising the plan — just to make sure we choose the safest next step."
Use this phrase directly with patients — it normalises supervision rather than making it look like failure.
📁 Your Portfolio Routine — Every 1–2 Weeks
Do not wait for panic. A steady fortnightly habit protects you at ARCP. The trainees who struggle at ARCP are rarely those who lacked effort — they are those whose evidence was scattered, unmapped, or produced in a last-minute rush.
Upload evidence while fresh
Memories fade. Log while it is still vivid.
Write a short, meaningful reflection
One page of real insight beats five pages of description.
Map to capabilities deliberately
Check which of the 13 capabilities each entry covers.
Update your PDP as patterns emerge
A PDP written at the start and never revisited is not a PDP — it's a memory.
Check capability coverage gaps
Some capabilities are easy to forget (e.g. OML, ethics, fitness to practise).
Build towards your ESR continuously
Your ESR needs self-ratings, evidence, PDP updates, and action plans — not a panic the week before.
🚨 Red Flags & Safety
The presentations you must not miss in general practice. Organised by system so you can scan fast and act faster.
Neurological
Cardiovascular
Respiratory
Gastrointestinal
Paediatric
Cancer 2WW
Medico-Legal
Unsafe Assumptions
⚖️ Safety-Netting — Medico-Legal Principles
- → Safety-netting must be documented in the notes — use SNOMED codes where available
- → Verbal safety-netting alone is insufficient in complex cases — provide written information where possible
- → Chase outstanding investigations — you have a duty to follow up results and communicate them
- → Track hospital referrals — if a patient does not attend, contact them and document
- → When in doubt — arrange review; do not just hope it resolves
🛡 Gold-Standard Safety-Net — FIRM
| Letter | What it means |
|---|---|
| F — Find | Name the specific red flag symptoms to watch for |
| I — Inform | Give an exact expected improvement timeframe |
| R — Return | Tell them exactly when and where to return |
| M — Make specific | Never just say "come back if worried" |
⚠️ Common Pitfalls
These are the mistakes that repeatedly catch trainees out — in their GP posts, their ePortfolios, and their ARCP reviews. Read them once. Remember them always.
🚨 Pitfalls That Cost Trainees Their ARCP Outcome
- Leaving all WPBAs until the final month. Last-minute assessments are easy to spot — and they suggest you are not an autonomous learner who takes the process seriously.
- Writing log entries that are pure description. A narrative of what happened is not a log entry — it is a story. Log entries need reflection, self-analysis, and explicit evidence of learning (using ISCE).
- Not covering all 13 Professional Capabilities. A single-capability ePortfolio fails trainees at ARCP. Review your coverage early and fill gaps deliberately.
- Treating your CSR and ESR as a formality. Prepare properly. Allow 2–3 hours for your ESR prep. A thin, rushed ESR tells the panel you do not value the process.
- Leaving OOH sessions until the last GP post. This is a serious planning failure that creates enormous stress in ST3 and looks poor on your ePortfolio.
- Not doing the QIA/QIP in ST1. The QI project is mandatory every training year. ST1 is the easiest time to do it. ST3 is almost impossible with MRCGP exams happening simultaneously.
- Altered or retrospectively edited clinical records. All medical systems log every keystroke with a timestamp. Never alter records retrospectively — add a new, clearly dated note instead.
⚠️ Pitfalls That Slow Progress
- Coasting through ST1 because "it's the easy year." The trainees who build strong habits in ST1 thrive in ST3. The ones who coast arrive in ST3 underprepared — with the MRCGP waiting for them.
- Expecting your trainer to remind you about WPBAs. They will not. They are training you to be an autonomous learner. This responsibility is yours.
- Waiting until you "feel ready" to record consultations for COTs. You will never feel completely ready. Start recording early, watch them back honestly, and use them as a learning tool — not just an assessment hurdle.
- Writing log entries only about things that went badly. Positive experiences with genuine reflection are equally valid. A pattern of only negative logs can inadvertently suggest poor practice rather than good self-awareness.
- Ignoring the typing skills problem. If you type slowly, every consultation and every log entry takes longer than it needs to. This is a fixable problem — TypingClub.com is free and genuinely effective.
- Not asking for the CSR to be completed. It will not happen automatically. Chase your trainer politely but directly.
🗣 Consultation Pitfalls
- History overload, management underload. The Clinical Management domain is weighted more heavily. Spending 9 of 12 minutes on history and rushing the plan makes it almost impossible to pass.
- Generic management plans. "We could try lifestyle changes first" without any specificity fails the management domain. Plans must be tailored to the patient's ICE, context, and comorbidities.
- Devolving clinical responsibility to ARRS colleagues. Saying "I'll refer you to the social prescriber/pharmacist/physio" without managing anything yourself signals unsafety. Applying NICE guidelines is your job.
- Circular or repetitive questioning. "Any weight gain? Any weight loss?" separately — when "any change in your weight?" covers both. Examiners notice question inefficiency.
- Ignoring non-verbal cues. When the patient pauses, looks worried, or changes tone — and you plough on regardless — you lose marks in the Relating to Others domain.
- Rereading history already in the opening notes. This wastes time and annoys examiners. Read the pre-consultation information carefully before the case begins.
- IMG-specific pitfall: WPBA is equally weighted with AKT and SCA in the MRCGP assessment. Many IMGs over-invest in written exam preparation and under-invest in ePortfolio entries — this creates a real risk of an unsatisfactory ARCP outcome even when exam performance is good.
🗣 Starter Consultation Phrases
Natural, adaptable phrases drawn from consultation skills literature and UK GP training resources. Memorise the principle, not a script — then adapt to your own voice and the patient in front of you.
🚪 Opening & Agenda-Setting
- → "What would you like to talk about today?"
- → "Before we dive in — what were you hoping I could help with today?"
- → "How have things been going since we last met?" (follow-up)
- → "Is there anything else on your mind that you wanted to bring up today?"
💭 Establishing Ideas (ICE — Thoughts)
- → "What thoughts have you had about what might be causing your symptoms?"
- → "What's your brain been telling you?"
- → "Some people in this situation wonder if it might be something more serious — has anything like that crossed your mind?"
- → "I just wonder what ideas you've had about what it might be?"
😰 Establishing Concerns (ICE — Worries)
- → "Is there something at the back of your mind that you're particularly worried about?"
- → "What is the worst thing you think this might be?"
- → "Have you looked anything up? What did you find?"
- → "What is it that particularly concerns you about this?"
🙋 Establishing Expectations (ICE — Help/Hopes)
- → "What were you thinking we could do about it today?"
- → "What were you hoping might come from today's appointment?"
- → "What else have you thought about?"
🤝 Empathy — Interpretive, Not Generic
Interpretive empathy names the specific emotion and links it to the patient's situation. Generic empathy is less powerful.
- → "That must be really hard for you, especially with everything else going on at home."
- → "You've clearly been through a lot — and now this on top of it."
- → "It sounds like a very worrying time."
- → "I think most people would feel the same way in your position."
➡️ Signposting to Management
- → "Shall we explore some of the ways we can approach this?"
- → "Would it be alright if we moved on to talking about what we can do to make things better?"
- → "Based on what you've told me, the most likely explanation is [X] — I'd like to go through what that means and what options we have."
💬 Explaining & Reasoning
Lead with evidence, arrive at diagnosis — the patient anticipates rather than argues.
- → "You have [these features], which is reassuring because it doesn't fit with anything serious — so what I think is going on here is [X]."
- → "I think what's going on here is [X] because of [Y] and [Z]."
- → "I'm reassured by the absence of [red flag] — that makes me less worried about anything sinister."
🤔 Handling Uncertainty
- → "I want to be honest with you — I don't know for certain yet, but the most likely explanation is [X]."
- → "I think this is most likely [X], but I want to rule out [Y] as well, and here's how I'd do that."
- → "It's sometimes not possible to be completely sure straightaway — but here's what I'd suggest we do to get more clarity."
🤜🤛 Shared Decision-Making
- → "There are a few options here — let me explain them and we can decide together what fits you best."
- → "How do you feel about that? Is that something you'd be happy to try?"
- → "Is there anything that would make that plan harder to manage for you?"
- → "The options are A, B, or C. What would you prefer?"
🛡 Safety-Netting — Specific & Actionable
Word order rule: End on a positive expectation — the last thing said is best retained.
- → "If [specific symptom] happens, or if you're not improving by [specific timeframe], please come back — or go to A&E if it feels urgent. But I expect you'll feel better within [X] days."
- → "I'd like you to call us if [red flag] develops — but I think these tablets should sort things out for you."
- → "Do come back if things aren't settling — but based on what you've described, I think nature will sort it out within the next week or so."
✅ Checking Understanding
- → "Just to make sure I've explained that clearly — what's your plan if things don't improve?"
- → "When you get home and someone asks you about today, what are you going to tell them?"
- → "Does that all make sense? Any questions about what we've agreed?"
💡 Insider Pearls
These are the insights that experienced trainees and trainers wish someone had told them at the start. Not in any guideline. Not in the RCGP curriculum. But true.
-
Your log entries are your only voice at ARCP. When a panel of people who have never met you sit down to decide whether you progress, they hear your voice through your log entries. Make sure it sounds like a thoughtful, reflective, developing doctor — not a box-ticker writing summaries of clinic.
-
The first three months feel hard — and that is completely normal. Moving from hospital medicine to general practice is a bigger culture shift than most trainees expect. The undifferentiated presentations, the brevity of consultations, the isolation of decision-making — all of it is genuinely challenging. You will adapt. Everyone does. Give yourself permission to find it difficult without concluding that you are failing.
-
Quality beats quantity in WPBAs. A few deeply reflected, well-discussed assessments are more valuable than a dozen that were rushed through just to tick the box. Your Educational Supervisor can tell the difference instantly.
-
Use FourteenFish as a reflection tool — not just an assessment repository. The trainees who engage most meaningfully with the ePortfolio often say it becomes genuinely useful for their own development — a place where they process what they are learning and track how they are growing. If it feels purely like bureaucracy, something is wrong with how you are using it.
-
The consultation gets faster as you get better at it. In the early weeks, a 15-minute slot can feel like trying to run a marathon in a corridor. As your consultation skills develop — through reading, reflection, and practice — the same slot begins to feel spacious. The skill is in efficiency of communication, not rushing through clinical content.
-
Get to know the whole team — including the "non-clinical" staff. The receptionist who knows which patients are likely to be difficult. The HCA who notices something unusual about a patient's appearance. The practice pharmacist who catches your prescribing error. These people are clinical assets, and building genuine relationships with them makes you a safer and more effective doctor.
-
If you trained abroad, the NHS hierarchy is flatter than you might expect. In UK general practice, GPs treat all colleagues — clinical and non-clinical — as equals within their domains of expertise. The expectation is mutual respect, not hierarchy. This is not just cultural guidance — it is assessed in your MSF.
-
Your PDP should reflect what actually needs developing — not what sounds impressive. A SMART PDP goal of "improve my knowledge of contraception by attending a family planning course by March" is far more powerful than "develop as a clinician." The former is achievable and shows self-awareness. The latter is vague and tells your Educational Supervisor nothing useful.
-
It is okay to debrief difficult consultations. Some consultations leave you unsettled — a complaint, a missed diagnosis, an angry patient, an unexpected death. These are the highest-value log entries. Processing them through the ISCE structure, discussing them with your trainer, and finding the learning in them is exactly what professional development looks like at its best.
-
PUNs and DENs — your personal AKT revision list. After each surgery, note 1–2 things you didn't know (Patient Unmet Needs / Doctor Educational Needs). These map directly to your AKT knowledge gaps and make powerful WPBA log entries. The trainees who do this routinely arrive at the AKT with far fewer surprises.
-
Use NICE CKS after every wrong AKT practice question. For each question you get wrong on Passmed or similar, go directly to the relevant NICE CKS page. This builds clinical knowledge in clinical context — not as isolated facts. It is substantially more effective than re-reading the question explanation alone.
-
AKT statistics: repeat the admin/stats section three times. Written knowledge for statistics cements faster with repetition than clinical topics. Trainees who maximise the statistics and organisation domains (20% of the AKT combined) consistently outperform those who focus only on clinical content.
-
SCA preparation: practise with multiple different people. Your usual study partner knows your consulting style and adapts to it. Varied consultation partners — who challenge you with unexpected responses, tears, or anger — build the adaptability that the real exam requires. This is one of the most commonly reported differences between those who pass first time and those who don't.
-
Train with 8-minute SCA consultations. Practising with an 8-minute constraint trains pace and forces ruthless prioritisation. When you return to the real 12-minute exam, it feels spacious rather than pressured. The management plan stops getting squeezed out.
-
In the SCA: make decisions. GPs make decisions based on probability even when uncertain. Examiners are specifically frustrated by trainees who gather a great deal of information and then refuse to commit to a plan. "I think this is most likely X, but I want to check Y" is confident and safe. "I'm not sure — we'll need more tests" without a working hypothesis is not.
-
Real listening scores more than model phrases. Genuinely pausing after the patient speaks, reflecting their words back, and responding to what has actually been said scores more Relating to Others marks than any perfectly executed ICE formula. Examiners have seen every phrase in every consultation skills book. They have not seen everyone use them with genuine attention.
-
The trainees who struggle at ARCP are rarely those who lacked effort. They are those whose evidence was scattered, unmapped, or produced in a last-minute panic. A portfolio full of well-reflected, capability-mapped entries from fortnightly habit beats a portfolio crammed with rushed entries in the week before the review panel — every time. Build the habit now.
-
Early GP difficulty is often less about medicine and more about NHS systems literacy. EMIS, Docman, Accurx, local referral pathways, prescribing rules, follow-up arrangements, and community team boundaries — none of these are taught in medical school. The fastest way to learn them is not to ask the same question twice. Write it down, learn it once, and build your own local reference.
For International Medical Graduates
If This Is Your First NHS-Style Primary Care Post
This section is for you — and it is honest, not condescending.
✅ What you ARE expected to do
- → Ask when you do not know a local pathway
- → Learn the system once — and retain it
- → Escalate when uncertain, early rather than late
- → Treat every colleague as an equal regardless of role
- → Accept supervision as normal, not shameful
❌ What you are NOT expected to do
- → Know every local pathway in week one
- → Consult at full speed from day one
- → Know the NHS bureaucracy instinctively
- → Be completely independent before you are ready
- → Mask uncertainty to appear more confident
💬 Communication in the early weeks
- → Clarity beats impressive vocabulary every time
- → Short sentences beat long explanations
- → Summarise back what you think the patient means
- → Check understanding before closing
- → If you are unsure what a patient said — ask them to repeat it, calmly
🧠 The emotional reality
- → Early GP can feel isolating — you make decisions with less immediate backup than in hospital
- → Feeling "behind" in the first 3 months is almost universal — it is not evidence of failure
- → Your first goals are safety, structure, and understanding the local system. Speed comes later.
- → The safest response to uncertainty is containment, documentation, follow-up, and asking early — not speed
🎓 Trainer & Teaching Pearls
Guidance for GP trainers and TPDs — common blind spots, high-yield tutorial ideas, reflective questions for both GP and hospital posts, and three ready-to-use teaching cases.
🔍 Common Trainee Blind Spots at This Stage
- Trainees frequently misunderstand the purpose of log entries — writing descriptions rather than reflections. The most effective early intervention is sitting with a trainee and reading a log entry together, then asking: "What did you actually learn from this, and what will you do differently?"
- The distinction between Achieving and Progressing in WPBA confuses many trainees — they assume anything short of "achieving" means failure. Clarifying this distinction early prevents unnecessary anxiety and misdirected effort.
- Many trainees, particularly IMGs, are unfamiliar with the expectation that they will take ownership of their training — requesting assessments, booking study leave, initiating tutorials. Explicitly naming this expectation at the outset prevents resentment on both sides.
💬 Tutorial Ideas for ST1/ST2 in GP
- Placement Planning Meeting: Use the four pillars (Relationships, Decision-Making, Management, Professionalism) as a framework. Ask the trainee: "Which of these feels most challenging to you right now — and why?" The answer tells you where to focus.
- Log entry review session: Ask the trainee to bring their best log entry and their weakest one. Reading and discussing both together — using the ISCE framework — is one of the highest-yield educational activities in ST1.
- COT before and after: Review a recorded consultation at week 4 and again at week 20. The growth in consultation fluency is usually visible and motivating for the trainee.
- Debrief as teaching: A structured post-surgery debrief — "what went well, what would you do differently, what did you learn?" — is a tutorial in miniature. Even 10 minutes of high-quality debrief is more valuable than 60 minutes of didactic teaching on a topic the trainee did not choose.
❓ Reflective Questions for Your Tutorials
- "If I were an ARCP panel member reading your ePortfolio today, what picture would I form of you as a developing doctor?"
- "Which of the 13 Professional Capabilities feels least well-evidenced right now — and what is your plan to address that?"
- "Tell me about a consultation this week that you keep thinking about. What is it about that consultation that you haven't fully resolved?"
- "What does a good day in general practice feel like for you — and what gets in the way of that on the bad days?"
- "If you imagine yourself at the end of ST3 — competent, confident, ready to practise as a GP — what would need to change between now and then?"
🏥 Reflective Questions for Hospital Post Tutorials
- "If this patient had presented to a GP rather than attending A&E, what would a safe and appropriate management plan have been?"
- "What long-term prescriptions did this patient have — and were they all still appropriate? What monitoring was overdue?"
- "Where did communication break down in this patient's care? What could have been done differently at the primary care stage?"
- "What did this patient not understand about their own condition — and how would you explain it in a 10-minute GP consultation?"
- "Was this admission preventable? What community resources might have helped?"
- "What aspect of this case did not fit the textbook? How do you manage uncertainty in clinical practice?"
🚩 Early Warning Signs in ST1 Trainees
- Over-confidence in clinical decision-making — calling for advice less and less, but making less sound decisions rather than better ones
- Log entries that are consistently descriptive and show no progression in reflective depth despite feedback
- Avoidance of recorded consultations for COTs — often signals a fear of being observed rather than laziness
- Poor engagement with the wider team — particularly with non-clinical staff
- Signs of significant stress or personal difficulty that are affecting clinical performance — these need gentle, direct conversation early
🎭 Teaching Case Scenarios
Three ready-to-use tutorial cases covering AKT-style clinical reasoning, SCA consultation skills, and medico-legal decision-making. Use these as discussion starters or written exercises.
🧠 Memory Frameworks & Mnemonics
The frameworks that make clinical knowledge stick and consultation skills automatic. Learn the structure — the content follows.
🧩 The GP Survival Model — SAFE → SENSIBLE → SHARED → SUPPORTED
Every good GP consultation maps onto these four words. Check each one before you close.
SAFE
- ✓ Red flags excluded
- ✓ Risk assessed
- ✓ Danger ruled out first
SENSIBLE
- ✓ Working diagnosis made
- ✓ Reasonable plan
- ✓ Not over-investigated
SHARED
- ✓ Patient involved in plan
- ✓ ICE addressed
- ✓ Explanation given
SUPPORTED
- ✓ Safety-net in place
- ✓ Follow-up arranged
- ✓ Documented clearly
💬 ICE — Reframed as TWH
Never use the words "ideas," "concerns," or "expectations" out loud — they sound clinical and scripted. Use TWH instead:
| Letter | Stands for | Natural phrase |
|---|---|---|
| T | Thoughts | "What has been going through your mind?" |
| W | Worries | "Is there something you are particularly worried about?" |
| H | Help/Hopes | "What were you hoping I might be able to do for you today?" |
🛡 FIRM — Safety-Netting Framework
Use FIRM to make every safety-net specific and scoreable:
| Letter | Stands for | What to say |
|---|---|---|
| F | Find the red flags | Name specific symptoms to watch for |
| I | Inform of timeline | Expected timeframe for improvement |
| R | Return if not improving | When and where to seek help |
| M | Make it specific | Not vague — not just "come back if worried" |
🏛 SOCRATES — Pain History
| Letter | Stands for |
|---|---|
| S | Site |
| O | Onset |
| C | Character |
| R | Radiation |
| A | Associated symptoms |
| T | Time course / pattern |
| E | Exacerbating / relieving factors |
| S | Severity |
🚨 SNOOP4 — Headache Red Flags
Any of these features = headache requires urgent investigation. Memorise SNOOP4 and use it every time a patient presents with headache.
🦠
SSystemic symptoms or disease (fever, weight loss, known cancer or immunosuppression)
🧠
NNeurological deficit (focal weakness, altered consciousness, papilloedema)
⚡
OOnset sudden / thunderclap → SAH until proven otherwise
👴
OOlder patient — new onset headache over age 50 → consider GCA, intracranial pathology
📈
PPrevious headache — change in character or frequency from baseline
⬆️
PPostural component — worse lying down / on standing → raised or low ICP
💨
PPrecipitated by Valsalva (cough, straining, sneezing) → raised ICP, Arnold-Chiari
📊
PProgressive — worsening over days to weeks → space-occupying lesion, subdural
🧩 TRAP — Parkinson's Disease Features
The four cardinal features. All four are tested in AKT and SCA. A patient needs at least two for a clinical diagnosis of Parkinson's, including bradykinesia.
Tremor
Resting "pill-rolling" tremor
4–6 Hz
Decreases with movement
Rigidity
Cogwheel (with tremor) or lead-pipe (without)
Affects all directions
Akinesia
Bradykinesia — slow initiation
Required for diagnosis
Micrographia, hypomimia
Postural Instability
Late feature
Loss of righting reflexes
Festinating gait
GP management: Refer to neurologist for diagnosis confirmation. First-line treatment in UK: levodopa (most effective for motor symptoms), dopamine agonists (pramipexole, ropinirole) — choice depends on age and risk of dyskinesias.
AKT pitfalls: Metoclopramide and prochlorperazine worsen Parkinson's — avoid in these patients. Drug-induced Parkinsonism (e.g., from antipsychotics) is reversible — does NOT respond to levodopa.
🧵 THREADS — Frailty & Falls Assessment
A structured aide-memoire for the multidimensional assessment of frailty and falls risk — directly maps to the RCGP Older Adults Topic Guide and is GP-exam relevant.
Mini-Cog or MMSE; delirium superimposed on dementia; medication effects on cognition
Correctable causes; hearing aids fitted correctly; visual acuity with glasses; cataracts
Polypharmacy; anticholinergics, benzodiazepines, antihypertensives → fall risk; STOPP/START criteria
Timed Up and Go (TUG) test; postural hypotension; Romberg test; gait assessment
Footwear; calluses, nail problems; arthritis limiting mobility; hip/knee OA
End-of-life anticipatory care planning; PHQ-2/9 for depression; reduced motivation → inactivity → falls
Postural hypotension (BP lying and standing); arrhythmias; Parkinson's; peripheral neuropathy; TIA/stroke history; carotid sinus hypersensitivity
📊 SnNout & SpPin — Statistics
| Rule | What it means |
|---|---|
| SnNout | High Snsitivity → Negative test rules out the diagnosis |
| SpPin | High Specificity → Positive test rules in the diagnosis |
🚗 DVLA Seizure / Epilepsy Driving Rules
One of the most consistently tested AKT Organisation & Management topics. Learn both the Group 1 (car) and Group 2 (HGV/bus) rules — they are completely different.
🚗 Group 1 — Ordinary Driving Licence (Car)
| Situation | Off Driving |
|---|---|
| First unprovoked seizure | 6 months |
| Established epilepsy (seizure-free) | 12 months |
| Seizure only during sleep (nocturnal pattern) | 1 year of sleep-only pattern |
| Withdrawal of AED | 6 months from stopping |
🚛 Group 2 — HGV / Bus / Coach Licence
| Situation | Off Driving |
|---|---|
| First unprovoked seizure | 5 years |
| Established epilepsy (seizure-free) | 10 years off AED |
| Nocturnal seizure pattern | Not eligible to hold licence |
📖 Consultation Models — Summary & Comparison
GP training uses several consultation models. You do not need to memorise every model — you need to understand what each one contributes and when to reference it in a COT, log entry, or SCA.
| Model | Core Concept | GP / SCA Relevance |
|---|---|---|
| Calgary-Cambridge | Task-based; 73 communication skills mapped to 5 consultation tasks (initiating, gathering, physical examination, explaining, closing) | Most commonly taught in UK GP training; RCGP assessment framework is built on this |
| Roger Neighbour (The Inner Consultation) |
5 checkpoints: Connecting → Summarising → Handover → Safety-netting → Housekeeping | Safety-netting originates here; "housekeeping" = managing your own emotional response after difficult consultations |
| Pendleton | Presenting problem → cause → predisposition → agreed action → patient understanding → resources available → patient involvement | Systematic but less flexible; used for structuring feedback in COT discussions |
| Balint | "The doctor as a drug" — the therapeutic relationship itself has healing power; emphasis on the doctor's own feelings | Relevant for complex, chronic, or emotionally demanding consultations; Balint groups used in GP training for reflective practice |
| SPIKES | Setting → Perception → Invitation → Knowledge (warning shot + news) → Emotion → Summarise/Strategy | Breaking bad news in SCA; use when delivering a serious diagnosis or unexpected result |
For your COT
Calgary-Cambridge provides the language for COT feedback. Know the 5 tasks so you can identify which part of the consultation to improve.
For your log entries
Neighbour's "housekeeping" checkpoint gives you a framework for reflecting on the emotional impact of consultations — a rich source of log entry material.
For SCA bad news cases
SPIKES gives you a clear sequence: set up → check what they know → check what they want to know → warning shot → news → respond to emotion → summarise plan.
🎯 Key Clinical Thresholds to Memorise
Memorise these specific numbers. The AKT tests thresholds repeatedly — knowing them cold saves time and marks.
🩺 Clinical Decision Thresholds
| Scenario | Threshold / Action |
|---|---|
| ABCD2 score ≥4 (TIA) | Same-day specialist review |
| CHA₂DS₂-VASc ≥2 (men), ≥3 (women) | Anticoagulate in AF |
| AUDIT-C ≥5 (alcohol) | Brief intervention |
| PHQ-9 ≥10 | Consider antidepressant |
| eGFR <30 | Stop metformin |
| Serum lithium target | 0.4–1.0 mmol/L |
| TSH suppressed on levothyroxine | Risk of AF + osteoporosis |
| ACEi — U&E monitoring | 1–2 weeks after each dose change |
📅 Screening Programme Ages
| Programme | When |
|---|---|
| Cervical screening (England) | Start age 25 · 3-yearly to 49 · 5-yearly to 64 |
| AAA screening | One-off USS at age 65 in men |
| Bowel cancer (qFIT) | Every 2 years, ages 50–74 |
| Breast screening | Mammogram every 3 years, ages 50–70 |
⚡ Rapid Recall — Colour-Coded by Urgency
🔴 Act Today
- ABCD2 ≥4 → same-day
- eGFR <30 → stop metformin
- SpO₂ <92% → admit
🟡 Watch Carefully
- TSH suppressed → AF/osteo risk
- Lithium 0.4–1.0 → toxic above
- PHQ-9 ≥10 → consider Rx
🔵 Routine Action
- AUDIT-C ≥5 → brief intervention
- CHA₂DS₂-VASc ≥2/3 → anticoagulate
- ACEi → U&E at 1–2 weeks
🟢 Screening Ages
- Cervix: starts age 25
- AAA: age 65 (men)
- Bowel: 50–74 / Breast: 50–70
❓ Frequently Asked Questions
The questions trainees actually ask — answered directly, without the bureaucratic run-around.
What is the minimum number of WPBAs I need to complete in a GP post? ▾
My trainer has not completed my CSR. What do I do? ▾
Do I have to do OOH sessions in ST1? ▾
How should my log entries be structured? ▾
What exactly is the QIA and when do I need to do it? ▾
What should I focus on in my Placement Planning Meeting? ▾
What do IMGs find most confusing or challenging about ST1 in GP? ▾
What happens if my ARCP goes badly? ▾
🏁 Final Take-Home Points
If you only remember ten things from this page, let them be these.
ST1 & ST2 in GP — The Bottom Line
Everything you need, in ten punchy points.
Understand the 13 Professional Capabilities before anything else. They are the frame on which everything hangs.
Write 1 log entry per week. Use ISCE. Show reflection, not just description. Quality beats quantity every time.
Your trainer will not remind you to do WPBAs. This responsibility is yours. Schedule them from week six onwards.
Do your QI project in ST1. Never in ST3. Your future self will send a thank-you card.
Start OOH sessions in every GP post — roughly one per month. Do not save them all for the last placement.
The ARCP panel may not know you. Your ePortfolio is your voice to them. Make it say something worth hearing.
ST1 feels hard in the first 3 months. That is normal. Your consultation fluency develops. Give it time and practice.
Read a consultation skills book this year. Communication skills are assessed in COTs, MSF, and the SCA exam.
Build real relationships with every member of the team — clinical and non-clinical. This is what MSF actually measures.
ST1 is your easiest year. Use it wisely. The habits, systems, and mindset you build now follow you all the way to CCT.
"The best GP trainees are not the cleverest ones — they are the most reflective, the most organised, and the most human. All three are learnable. And you have three years to learn them."
— Dr Ramesh Mehay, Bradford VTS
Bradford VTS — the universal GP training resource, free for all. Created by Dr Ramesh Mehay.
WPBA numbers verified against RCGP guidance (rcgp.org.uk/mrcgp-exams/wpba). Always check for updates.
Last updated: April 2026