Your GP Training Roadmap
Because knowing what you need to do — and when — is half the battle in GP training. The other half is actually doing it on time.
Last updated: April 2026
🌐 Web Resources
The key official links for GP training requirements and assessments.
🗺 The Big Picture
Three years. Two exams. One portfolio. Here is how it all fits together.
📌 What is this page about?
This page outlines the minimum WPBA assessments required at each stage of GP training (ST1, ST2, and ST3). Think of it as your training checklist — but with one important caveat built in from the start:
The minimum is the floor, not the ceiling. You should always be doing significantly more than the minimum — and spreading assessments throughout the year, not cramming them in at the end.
📊 WPBA Requirements at a Glance
ST1 and ST2 requirements are identical. ST3 is where things change.
| Assessment | ST1 & ST2 (per 6 months) | ST3 (per 6 months) |
|---|---|---|
| Every 6 months | ||
| Learning Log Entries | 24 minimum 18 of 24 must be Clinical Case Reviews | 24 minimum 18 of 24 must be Clinical Case Reviews |
| CBDs / CATs | ×2 minimum | ×2–3 CATs Min 5 by end of year (CBDs, RCAs, Referrals, Ix review) |
| COTs / Mini-CEX | ×2 minimum COT in GP post Mini-CEX in hospital | ×3–4 COTs Min 7 by end of year At least 1 Audio-COT |
| CEPS | As appropriate | All 5 mandatory by end of ST3 |
| Whole year | ||
| MSF | ×1 | ×2 MSF + Leadership MSF |
| LEA (significant event) | ×1 | ×1 |
| QIA | ×1 | ×1 |
| QI Project | ×1 If in a GP post | — |
| Leadership Project | — | ×1 |
| Prescribing Review | — | ×1 60 prescriptions |
| PSQ | — | ×1 Primary care only |
⏰ One Critical Deadline
Everything must be in your ePortfolio by the 34-month mark of training. The final 2 months are reserved for Educational Supervisor and ARCP panel meetings. Do not leave assessments to the last two months — your ES cannot sign you off without them.
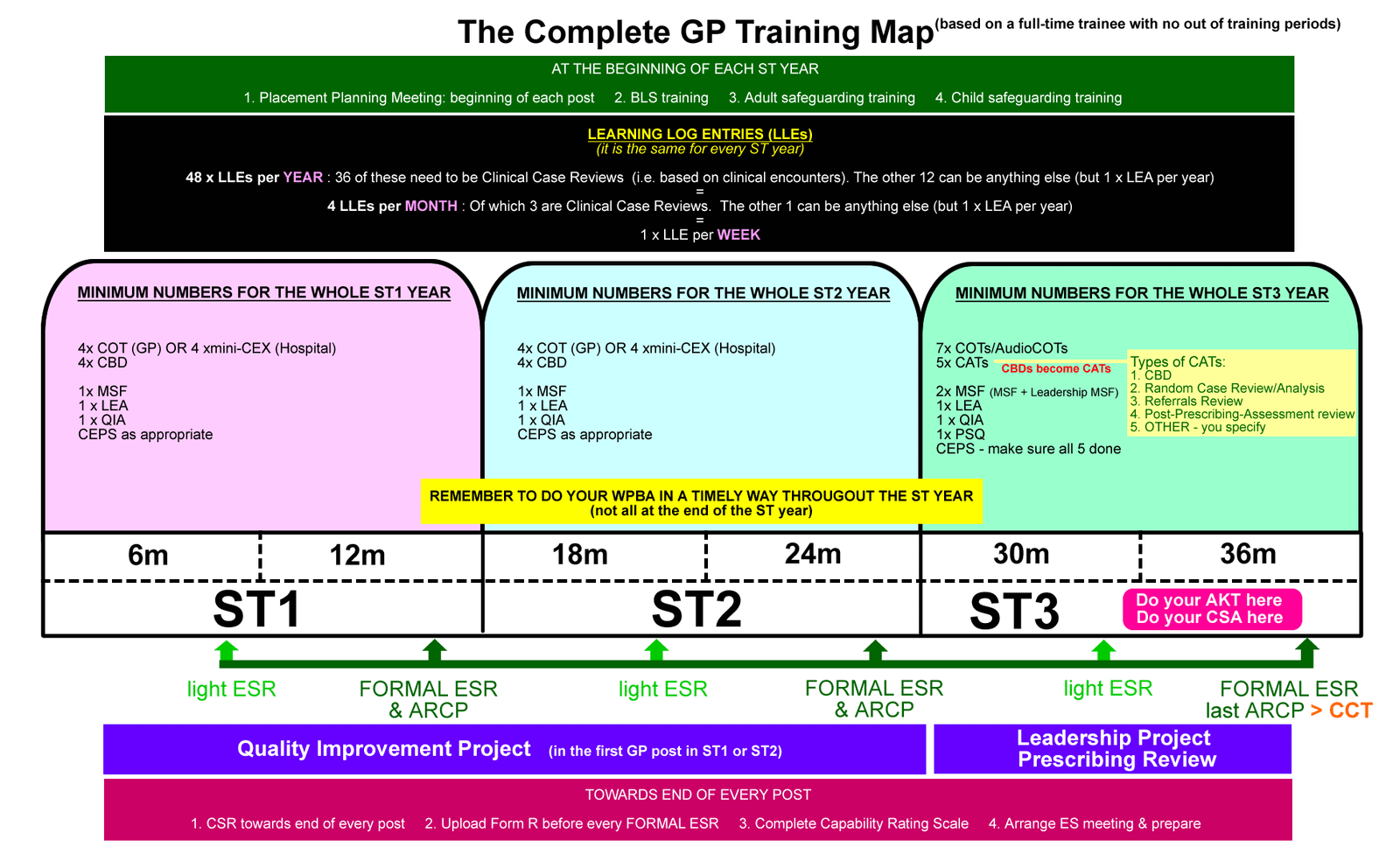
The full 3-year training map. Official RCGP guidance on numbers and timing →
🎯 When to Sit the Exams
AKT and SCA — the two MRCGP components you'll need to pass to complete training.
AKT
Applied Knowledge Test- Do not attempt before your first GP post in ST3
- Some clinical knowledge only comes from real GP experience — no amount of reading fully replaces it
- Aim for the beginning of your second 6 months in ST3
- Sit early enough to allow a resit if needed before 34 months
SCA
Structured Clinical Assessment- Can only be taken in ST3 — no earlier
- Use the first 6 months of ST3 to practise your consultation, clinical, and organisational skills
- Aim to sit at the start of your second 6 months in ST3
- The SCA tests knowledge and consultation skills — not just communication
💡 The Case for Sitting AKT and SCA Together
Many experienced GP educators recommend sitting both exams at roughly the same time — ideally at the beginning of your second 6-month ST3 post. The logic is simple: both exams require a strong clinical knowledge base. If you're revising for one, you're revising for the other. The knowledge is fresh, and you only have to go into "exam mode" once.
Don't leave it too late. You want time to resit if needed — and you want your final months of training to be about consolidation, not last-minute exam anxiety.
🤔 Not Sure Which to Do First?
There is no single right answer. Have a conversation with your trainer. They know your strengths, your learning style, and your progress. That conversation is worth more than any generic advice on a webpage — including this one.
📌 WPBA Ground Rules
Five things to know about assessments before you start organising them.
You are responsible
You decide when assessments happen — not your trainer, not your consultant. Organise them yourself, tell your supervisor when you're ready, and take ownership of the process. This is good practice for annual GP appraisal, where you'll do exactly the same thing for the rest of your career.
Give adequate notice
Ask your trainer or hospital consultant in advance — a week ahead is courteous. Don't try to squeeze all your assessments into the final fortnight of a post. No one will thank you for it, and the quality of feedback will suffer.
Help your hospital consultants
Hospital specialists may be unfamiliar with GP-specific assessments and competency frameworks. That's completely understandable — it is not their world. So help them. Understand the assessments yourself well enough to guide them gently if they're unsure. You'll both get more out of it.
"Needs Further Development" is normal
In ST1 and ST2, "Needs Further Development" is the expected grade for many assessments. If you're getting all "Competent" or "Excellent" grades in your first year, your trainers might actually be more worried — it could mean the cases are too easy, or the feedback is not honest. Development takes time. Embrace it.
Complete before your ES meeting
All assessments must be in your ePortfolio at least one month before your post ends. Your Educational Supervisor cannot complete their review or sign you off if the evidence is not there. The minimum is the minimum — not a suggestion. And remember: you should always be aiming to do more.
🔍 WPBA Component Notes
Specific guidance on each assessment type — what they are and how to approach them.
📖 Learning Log Entries ▾
Write approximately one log entry per week. Of your 24 minimum entries per 6 months, 18 must be Clinical Case Reviews — these are learning reflections on actual clinical encounters with patients. (Think of them as "clinical encounters" — the original term was arguably clearer.)
You can still write logs about learning from HDR sessions, reading, or wider reflections — but these don't count towards your 36 Case Review logs per year.
Struggling with format? Try Ram's easy method for writing learning logs — it turns a potentially painful task into something quick and genuinely useful.
💬 CBDs and CATs (Case-Based Discussion / Consultation Assessment Tools) ▾
Preparation matters. Don't select a case at the last minute. Case selection is important — different cases let you demonstrate different Professional Capabilities, and you need to cover them all to complete training. Plan ahead and choose cases that fill your gaps.
In ST3, "CATs" is the broader term covering CBDs, RCAs (Referral Case Audits), Referral Reviews, and Investigation Reviews. You need a minimum of 5 CATs by the end of your ST3 year.
🎙 COTs (Consultation Observation Tools) and Mini-CEX ▾
COTs are done in GP posts; Mini-CEX assessments are done in hospital posts. Don't confuse the two — a Mini-CEX does not count as a COT, and vice versa.
In ST3, you need a minimum of 7 COTs by the end of the year — including at least one Audio-COT, where your consultation is recorded and reviewed. This gives you and your trainer detailed feedback on your consultation style, pacing, and structure.
📝 CEPS (Clinical Evaluation of Procedural Skills) ▾
There are 5 mandatory CEPS to complete by the end of ST3. Hospital posts are often a good opportunity to get many of these done, as you'll have more access to certain practical procedures.
Don't leave these to your final GP post — some may not arise naturally in a GP setting, and scrambling at the end is stressful.
👥 MSF (Multi-Source Feedback) ▾
In hospital posts, your MSF raters will be clinical colleagues only. In primary care, both clinical and non-clinical raters (receptionists, admin team, nurses) are included. This reflects the full range of people you work alongside in general practice.
In ST3, you need two MSFs — your standard MSF and a Leadership MSF. These are separate tools assessing different dimensions of your professional behaviour.
🔍 LEA (Learning Event Analysis / Significant Event) ▾
One LEA per year is required. These are reflective analyses of significant events — things that went unexpectedly well, unexpectedly badly, or that offered an important learning opportunity. There is no strict minimum number of SEAs beyond one — but you should complete them as and when relevant events arise, not save them up artificially.
📊 PSQ (Patient Satisfaction Questionnaire) ▾
PSQs are only completed in the primary care setting — they cannot be done in hospital posts. This is a formal questionnaire distributed to patients to gather feedback on your consultations. Plan ahead so this is completed during your GP post in ST3 with enough time for results to feed into your ARCP evidence.
📋 CSR and Mid-Year Review ▾
The CSR (Clinical Supervisor's Report) does not need to be completed if the Clinical Supervisor is also the Educational Supervisor. This commonly applies to first GP placements in ST1 or ST2.
The Mid-Year Review is a lighter-touch ES meeting — a check-in to make sure you're on track. No formal ESR is generated, but your ES should write an Educator's Note covering: Good Points, Not-So-Good Points, and Things to Work On. Think of it as a progress conversation rather than a formal assessment.
✅ Final Take-Home Points
- The minimum numbers are a floor. Always aim to do significantly more, and spread assessments throughout the post.
- Everything must be in your ePortfolio by the 34-month mark — the final 2 months are for panel meetings, not last-minute uploads.
- ST1 and ST2 WPBA requirements are identical. ST3 has additional expectations: Leadership MSF, Prescribing Review, PSQ, Leadership Project, and Audio-COTs.
- You organise the assessments — not your trainer. Take ownership of this from day one.
- "Needs Further Development" is normal and expected in early training. It is not failure. It is the point.
- Aim to sit AKT and SCA at the beginning of your second 6-month ST3 post — early enough to resit if needed, but late enough to have real GP experience behind you.
- When in doubt about WPBA requirements or exam timing, speak to your trainer or TPD. Official guidance is on the RCGP website — always check there first.
Thank you so much for this. Very helpful