Planetary Health
Because looking after the planet is looking after our patients — and learning to see both at once is one of the most grown-up things a GP can do.
🎯 What you will learn from this page
Aim
To provide, in one place, a clear introductory guide to planetary health focused on the needs of UK GP trainees, trainers and TPDs.
Objectives
- Introduce the key concepts of planetary health in the RCGP curriculum.
- Review how climate change is affecting human health.
- Review how primary care itself contributes to environmental harm.
- Identify the clinical changes that protect both patients and the planet.
📥 Downloads
Handouts, summaries and teaching extras — ready when you are.
Web Resources
A hand-picked mix of official guidance and real-world GP training resources — because sometimes the best pearls are not hiding in the official documents.
🏛️ Core guidance & policy
- RCGP — Population & Planetary Health curriculum topic guide
- RCGP — Planetary Health & Sustainability in WPBA
- RCGP — Sustainable development, climate change & green issues (policy hub)
- NICE NG245 — Asthma: diagnosis, monitoring & chronic asthma management (2024)
- Five years of a Greener NHS: progress and forward look (NHS England, 2025)
- Delivering a Net Zero NHS — original 2020 strategy
- Greener NHS — Net Zero landing page
- RCGP Net Zero Hub — eLearning
🌱 Practical greener practice
💨 Air pollution & environment
One-Minute Recall
If you only read one thing on this page, read this.
The 10 things a GP trainee needs to know
- Definition: The RCGP topic guide frames planetary health as the health of human society together with the natural systems that make it possible.
- NHS carbon: The NHS accounts for around 4–5% of the UK's total carbon footprint and about 30–40% of all public sector emissions (NHS England, 2025).
- NHS progress: Direct NHS emissions have fallen 14% in the 5 years since the Net Zero strategy launched (NHS England, 2025) — the NHS is on track for its 2028–32 interim target.
- Primary care share: Primary care is responsible for about 23% of NHS England's emissions. Pharmaceuticals and chemicals account for nearly half of that.
- Biggest lever: Medications dominate primary care's carbon footprint. Waste disposal is only around 0.5%.
- Inhalers: Pressurised metered-dose inhalers (pMDIs) have a much higher carbon footprint than dry powder inhalers (DPIs) — roughly 40× higher per inhaler (Greener Practice). The UK is an outlier in Europe for pMDI use.
- Two questions: For every patient ask — how does the environment affect this person's health? and how does my management affect the environment?
- Four principles: Prevention · patient empowerment · lean pathways · low-carbon alternatives.
- Co-benefits: Active travel, plant-rich diets and social/green prescribing improve health and reduce emissions — double wins.
- Inequality is central: The richest 10% produce around half of global emissions, but the poorest suffer most from the harm.
- Air pollution kills: Around 38,000 deaths a year in the UK are attributable to air pollution (UKHSA). In December 2020 a UK coroner ruled air pollution contributed to the death of Ella Adoo-Kissi-Debrah — a world-first ruling.
What Is Planetary Health?
Planetary health, as framed in the RCGP topic guide, brings the connection between human wellbeing and the environment into the everyday clinical picture:
📖 The RCGP definition
The RCGP topic guide describes it as the health of human society together with the natural systems that sustain it.
Planetary health looks at health and healthcare through many lenses. It studies the interactions between human activity, our health, and the effects our healthcare has on the environment around us.
Climate change is the best-known part of this, but the story is bigger. The stability of life on earth also depends on staying within an ecological ceiling — a safe limit — for things like:
Chemical pollution
Including pharmaceuticals in waterways.
Freshwater withdrawal
Overuse of water for agriculture and industry.
Biodiversity loss
Loss of plant, animal and insect species.
Air pollution
Particulate matter, NOₓ, ozone, sulphur dioxide.
Nitrogen & phosphorus
Run-off from farming that harms waterways.
Ozone depletion
Damage to the atmospheric ozone layer.
Ocean acidification
CO₂ absorbed into the sea makes it more acidic.
This framework comes from Kate Raworth's Doughnut Economics. Think of it as two rings. The inner ring is the social foundation (the minimum people need for a decent life). The outer ring is the ecological ceiling (the limits the planet can cope with). A healthy society lives in the ring between the two.

💡 How to explain this to a patient (or a sceptical colleague)
"Our health doesn't sit inside our body alone. It sits inside our community, which sits inside our country, which sits inside the environment. If any of those layers is unwell, the next layer up will feel it too."
Why This Matters in GP
Planetary health is the overarching determinant of human health. We depend on the planet's life-support systems for our wellbeing and, ultimately, our survival. Understanding how natural systems interact with health is no longer optional — it shapes the conditions we see every day in clinic.
At the same time, providing healthcare has a carbon footprint of its own. The NHS accounts for around 4–5% of the UK's total carbon footprint and approximately 30–40% of all public sector emissions (NHS England, 2025). Primary care alone accounts for about 23% of NHS England's emissions, with pharmaceuticals and chemicals accounting for nearly half of that figure.
There is real progress too. Direct NHS emissions (the "NHS Carbon Footprint") have fallen by 14% in the 5 years since the Net Zero strategy launched, and the NHS is on track to meet its 2028–32 interim target (NHS England, 2025).
Much of what we do leaves a trace in the environment. Pharmaceutical waste and single-use plastics are particularly hard to break down. Pharmaceuticals are now commonly detected in freshwater, where they affect plants and animals.
Healthcare is both a cause and a consequence of environmental harm. The more we understand this, the more leverage we have to act.



💡 Why trainees should care
Planetary health is now explicitly in the RCGP curriculum. It is assessable through WPBA (CbD, COT, Leadership activities, and QIPs) and is a natural fit for ARCP evidence. Even more importantly, many planetary health actions are simply good medicine — less overtreatment, better shared decision-making, more prevention.
Core Concepts in the RCGP Topic Guide
The RCGP topic guide introduces several ideas that are useful in everyday GP work. The goal is not to memorise the greenhouse-gas potential of every inhaler brand, but to learn a different way of seeing your clinical work.
Planetary health and complexity
Planetary health reminds us that complex systems have many interacting parts, feedback loops and tipping points. We already know this from physiology — think of blood glucose control through hormonal and cellular loops. Planetary health simply zooms the lens out: how humans shape the world, and how the world in turn shapes us.
GPs are often more comfortable with complexity than hospital specialists, because we rarely meet patients with only one condition. We are trained to weigh up personal, social and environmental factors that change how disease affects a patient.
🔬 A useful distinction
Most evidence-based medicine comes from randomised controlled trials — which deliberately avoid complexity by excluding people with multiple conditions. RCTs told us which drugs reduced COVID-related mortality. Systems theory, in contrast, helps us understand why the pandemic spread the way it did and why some interventions worked for some populations. We need both.
Two questions to ask every day
If planetary health is so complex, how do we use it in a 10-minute consultation? Keep it simple. Two questions are enough:
❓ Question 1
How does the environment affect this patient's health?
Example: a child with asthma — is it being driven by air pollution from traffic, local industry, or mould in damp housing?
❓ Question 2
How does my management affect the environment?
Example: have I chosen inhalers that lower greenhouse gas emissions? pMDIs contain propellants that are 1,000–3,000× more potent than CO₂. DPIs contain none.
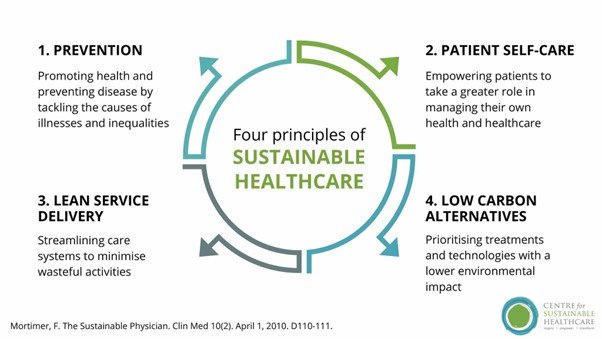
Four principles of sustainable clinical practice
The topic guide invites us to audit our work through four principles. They are simple, memorable, and surprisingly powerful once you start applying them.
We will go through these in detail in the next section.
Inequality, health and justice
Across planetary health, one pattern keeps repeating: the harm from environmental damage falls heaviest on those who have done least to cause it, and have the fewest resources to respond.
This is true internationally (the poorest countries suffer most from climate change) and locally (the poorest neighbourhoods suffer the worst air pollution and the poorest housing). It is the modern face of Tudor Hart's Inverse Care Law.
Dr Ram's Two Questions — A Consulting Habit Worth Building
Reading about planetary health is one thing. Using it in a real consultation is another. Here is a simple habit that takes about ten seconds and fits any consultation.
1️⃣ Does the environment affect this patient?
- Are they exposed to air pollution (main road, industry)?
- Is their housing damp, mouldy, or hard to heat?
- Could heat, cold or poor air quality be driving their symptoms?
- Is their diet, travel or lifestyle contributing?
2️⃣ Does my management affect the environment?
- Is this prescription actually needed?
- Is there a lower-carbon option (DPI vs pMDI)?
- Can I deprescribe anything?
- Could a non-medication approach work just as well (social, green or blue prescribing)?
🧠 Try this worked example — a young adult with mild asthma
Question 1: She lives on a busy road. Pollution is probably part of the picture. A conversation about indoor air, route to work, and active travel is worth having.
Question 2: She currently uses a salbutamol pMDI alone. Under NG245 (2024) this is no longer a recommended regimen. A review to move her onto an ICS/formoterol combination as as-needed AIR therapy (or MART if symptoms are more frequent) is indicated anyway — and the preferred DPI devices are substantially lower-carbon than pMDI alternatives.
One short consultation. Two questions. Two benefits: guideline-concordant, better-controlled asthma and lower emissions.
The Four Principles of Sustainable Clinical Practice
These four principles are the heart of the RCGP topic guide. Learn them, and you have a usable framework for every consultation.
Prevention
Prevent illness and promote health. The most sustainable healthcare is the healthcare a patient never needs. Smoking cessation, alcohol advice, vaccination, cancer screening.
Patient empowerment
Support patients to manage their own health through education, shared decision-making and self-care. Empowered patients consult less and use fewer resources.
Lean pathways
Give the right care to the right patient — and no more. Avoid low-value investigations, appointments or treatments that do not change outcomes.
Low-carbon alternatives
When treatment is needed, pick the option with the smallest footprint — for example DPIs over pMDIs, oral over IV where safe, local over distant referral where equivalent.

💡 The honest truth
These four principles are not new ideas dressed up in green clothing. They are things good GPs already try to do. Prevention, empowerment and lean pathways are the backbone of safe, patient-centred care. Planetary health just gives us an extra reason to take them seriously.
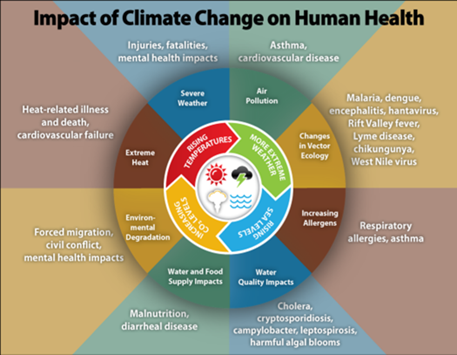
Impacts of Climate Change on Human Health
Climate change touches almost every part of medicine. Some effects are direct (heat, storms, air pollution). Some are indirect (disease spread, food supply, mental health). The clinical picture is layered and it is already here.
💨 Air pollution — see dedicated section below
Air pollution is covered in its own section because of its size and importance. Scroll down to Air Pollution.
🦟 Changing vector ecology
Vector-borne diseases have spread as the climate has warmed. Lyme disease has moved from being a localised condition (the New Forest in the UK) to being widespread across the country.
Dengue fever is an even bigger story. In 1970 it was present in 9 countries; today it is endemic in more than 100 (WHO). Local transmission has been reported in Europe since 2010.
🌾 Increasing allergens
Longer, warmer growing seasons mean more pollen, for longer. This is linked to worsening hay fever and asthma. Air pollution makes allergic responses more severe — a double hit (CDC).
💧 Water quality and diarrhoeal illness
Diarrhoeal diseases increase when temperatures are higher, and with both very high and very low rainfall. This matters globally far more than in the UK, but UK flooding events do disrupt water safety too (CDC).
🌽 Water and food supply
Deserts have enlarged in North Africa. Storm damage is making other farming regions less reliable. The UK's food supply depends on world markets, not local production — so distant shocks hit local prices hard. The 2022 Ukraine war showed this plainly (BBC; Al Jazeera).
In general practice this shows up as food poverty — a social determinant that affects nutrition, mental health, and adherence to advice about diet.
🌊 Environmental degradation and ocean acidification
Rising CO₂ does two things. It drives the greenhouse effect. It also dissolves into the oceans, making them more acidic. More acidic seas harm any marine life with a shell — corals, shellfish, and possibly the plankton that produce much of the world's oxygen (NHM).
Other degradation is more directly human — plastic waste, and pharmaceuticals that sewage treatment plants cannot fully break down. (See Sharon Pfleger's Greener Practice webinar — Medicines and the Environment.)
🏚️ Severe weather and mental health
Floods, storms and fires cause direct harm, damage to health infrastructure, and longer-term psychological effects such as PTSD and depression. Housing damage and mould cause further chronic harm.
Even people not directly affected can suffer from climate anxiety — a growing problem in young people (Lancet Planetary Health, 2021).
At the planetary level, severe weather is a major driver of migration, as farming and water supply fail. Migration then interacts with access to healthcare, housing, food and social support — all GP territory.
Air Pollution — The Quiet Epidemic
Air pollution is associated with about 7 million premature deaths worldwide every year, and up to 38,000 deaths a year in the UK are attributable to poor air pollution according to the UK Health Security Agency (NHS England, 2025). Its effects are not limited to the lungs — every organ is affected.
🚨 UK legal landmark (December 2020)
In December 2020, a UK coroner ruled that air pollution contributed to the death of 9-year-old Ella Adoo-Kissi-Debrah from asthma — believed to be the first time anywhere in the world that air pollution was listed as a cause of death on an individual death certificate. Ella had lived 25 metres from the South Circular Road in south-east London and had been exposed to levels of nitrogen dioxide and particulate matter above WHO guidelines. The ruling changed the legal and political weight of this conversation permanently.
What's actually in air pollution?
| Pollutant | What it is | Main harms |
|---|---|---|
| PM10 | Particles ≥10 nm — larger | Nose and throat irritation; upper airway disease. |
| PM2.5 | Fine particles ≤2.5 μm | Penetrate into cells; drive cardiovascular disease, stroke, cancer, developmental harm. |
| Nitrogen oxides (NOₓ) | From combustion — mostly vehicles | Respiratory disease, lung development, asthma exacerbation. |
| Sulphur dioxide | Fossil fuel burning | Airway irritation, bronchoconstriction. |
| Carbon monoxide | Incomplete combustion | Reduces oxygen delivery; cardiovascular and cognitive effects. |
| Ozone (O₃) | Secondary pollutant formed from NOₓ + sunlight | Inflammation, reduced lung function. |
Because real-world sources produce mixtures of these pollutants, it is hard to untangle the effect of each one. That mixing is also what produces ground-level ozone — a secondary pollutant that adds further harm (Clean Air Hub).

Data from 2021 shows that 35% of NOₓ and 13% of PM2.5 come from transport (gov.uk). Electric vehicles reduce NOₓ but still produce tyre and brake particles, so PM2.5 will fall less than we might hope.
Who does it affect?
Air pollution affects every organ and every life stage — from pregnancy and childhood development to heart attacks, strokes, diabetes, fertility and cognitive decline.


🚗 Common myth: "I'm safe in my car with the air-con on"
Not really. Research shows in-car pollution builds up from neighbouring vehicles and can reach concentrations higher than outside (RAC). Walk or cycle where you can — and use back roads.
🪵 Another quiet source: domestic log burners
Log burners are a preventable source of pollution that harms both the household using them and the downwind neighbourhood. Helpful advice from Clean Air Hub.
💡 Quick actions for you and your patients
- Check local air quality on apps or websites — take the Clean Air Hub calculator quiz.
- Avoid main roads for walking and cycling routes where possible.
- Think about air pollution as a cause for respiratory and cardiovascular consultations — not just a background issue.
- Advise patients about indoor sources too: log burners, smoking, cooking without ventilation.
- Patient info: Greener Practice — air pollution.
Direct Effects of Heat on Health
Heat is sometimes called a silent killer. Many heat-related deaths are only spotted retrospectively. Those most at risk are the people who are already vulnerable — the elderly, the frail, young children, pregnant women, homeless people, outdoor workers, and people with chronic disease (WHO).
The harm depends on both intensity and duration (including how warm the nights stay).

💊 Heat and common medications
Heat causes vasodilation as a physiological response, which puts strain on the circulation. Many common drugs — such as antihypertensives and diuretics — affect vasodilation or fluid balance in ways that may interact with this strain. Patients taking these medications during heatwaves may be at higher risk of dehydration, postural hypotension, falls and acute kidney injury. Follow UKHSA Adverse Weather and Health Plan guidance and local protocols. Any changes to a patient's medication regimen must be made on an individual basis following usual clinical assessment — never as a blanket instruction.
Severe weather
Floods, storms and fires cause immediate injuries and deaths, disrupt health infrastructure, and leave long psychological shadows. Climate anxiety is now a recognised phenomenon, especially in younger people (Lancet).
Clinical Changes That Reduce Carbon
Greener NHS data consistently show that medication is the biggest slice of primary care's carbon footprint. That means the most meaningful changes are clinical — how we diagnose, prescribe, and review.

🔍 Overdiagnosis and overtreatment
The RCGP Overdiagnosis Group defines it as applying labels and treatments that add little value or cause net harm. That framing shifts the conversation from "what is the matter with them?" to "what matters to you?" (What Matters to You).
Classic examples:
- An old "asthma" diagnosis made in A&E years ago, never reviewed — still generating inhaler prescriptions.
- A "hypertension" label based on one reading, followed by years of normal BPs.
- Overtreatment of borderline type 2 diabetes.
- Screening for conditions where the benefit is small and the downstream harm is large.
More: Greener Practice — overdiagnosis and person-centred medicine.
💊 Polypharmacy and deprescribing
The more medications a patient takes, the higher the risk of interactions and side effects — and the more likely it becomes that one drug exists only to treat the side effect of another. Assessing anticholinergic burden in frail or older patients is a useful starting point.
Around 50% of patients with chronic conditions do not take their medication consistently (NCBI, 2018) — but most still collect their prescriptions. That means the carbon has already been produced.
A good medication review is a clinical win and a carbon win. See Greener Practice — prescribing and deprescribing.
💚 Alternatives to tablets — green, blue and social prescribing
Historically we have prescribed tablets for conditions like anxiety and depression. Evidence now shows that for many people, talking therapies should be offered first-line or alongside medication where needed (NICE NG222).
- Green prescribing — time outdoors in nature.
- Blue prescribing — time near water.
- Social prescribing — connection, community, purpose.
Evidence for these is growing, especially for mental health (Challenges, 2019).
The inverse care law applies here too: good green and blue spaces are typically least available in the places that need them most.
Inhalers — The Single Biggest Carbon Lever in Primary Care
Inhalers deserve their own section because they dominate the prescribing carbon footprint. They are also a classic example of how better clinical care and lower carbon point in the same direction.
🌍 The numbers
- Most UK inhaler prescriptions have historically been pressurised metered-dose inhalers (pMDIs). The UK has been a European outlier for pMDI use — much higher than Sweden, for example.
- pMDIs contain hydrofluorocarbon propellants, with greenhouse-gas potency many hundreds to thousands of times that of CO₂.
- Dry powder inhalers (DPIs) and soft mist inhalers contain no propellant gases.
- Per inhaler, pMDIs produce roughly 40× the carbon footprint of DPIs (Greener Practice).
- UK asthma outcomes have been worse than several comparable European countries — so high pMDI use cannot be justified by superior outcomes.
The 2024 guideline change that reframes everything
In November 2024, NICE, BTS and SIGN published the combined national asthma guideline NG245. It represents a fundamental shift in how we manage asthma in people aged 12 and over — and a small but important change for children aged 5 to 11.
📋 What NG245 (2024) says (adults and young people aged 12+)
- Do not prescribe a SABA (short-acting beta₂ agonist) on its own for asthma. Every SABA must be paired with an inhaled corticosteroid (ICS).
- First-line for newly diagnosed asthma: as-needed AIR therapy — a low-dose ICS/formoterol combination inhaler used only when symptoms occur.
- If symptoms are more frequent or severe: low-dose MART (Maintenance And Reliever Therapy) — the same ICS/formoterol inhaler used both regularly and as the reliever. Patients on MART do not usually need a separate SABA.
- If asthma remains uncontrolled on low-dose MART, step up to moderate-dose MART. If still uncontrolled, trial an LTRA or LAMA before referral.
- Inhaler choice should take into account correct technique, patient preference, lowest environmental impact, and the presence of a dose counter.
- Digital inhalers are not recommended for routine use (NG245, 2024).
- Review response at 8 to 12 weeks after starting or changing treatment.
📋 What NG245 says for children aged 5 to 11
- Initial treatment: twice-daily paediatric low-dose ICS, with SABA as needed.
- Consider paediatric low-dose MART if asthma is uncontrolled on ICS + SABA and the child can manage a MART regimen.
- Only one budesonide/formoterol DPI was licensed for MART in this age group as of November 2025 — use of any other ICS/formoterol combination inhaler for MART in under-12s is off-label and requires informed discussion.
- If MART is not manageable, consider adding an LTRA for 8–12 weeks (follow MHRA safety advice on montelukast neuropsychiatric reactions).
⚠️ Why this matters for planetary health
AIR and MART are not just more environmentally friendly — the NICE economic analysis found them to be both more effective and less costly than SABA-only or traditional ICS-plus-SABA regimens. The licensed budesonide/formoterol inhalers used for AIR and MART include DPIs (such as Symbicort Turbohaler) which have a much lower carbon footprint than pMDI alternatives. Getting the clinical regimen right usually gets the carbon right too.
First rule: good clinical care always comes first
A patient with uncontrolled asthma does not need a greener inhaler — they need a working regimen. Most of the carbon savings in respiratory care come from better disease control and regimens in line with current NG245 guidance, not from device changes alone.
🧠 The SABA-overuse pattern
Historically, people using three or more SABA inhalers a year were flagged as having poor control. Under NG245 (2024), that pattern now prompts a complete review against the new treatment pathway — not simply a "top-up" of their existing regimen. Many of these patients should never have been on SABA alone.
How to reduce the carbon footprint of inhaler prescribing
Follow NG245 properly
Move eligible patients to AIR or MART regimens in line with the guideline. Most of the carbon benefit follows automatically.
Prefer lower-carbon devices
Where clinically appropriate and the patient can use it well, a DPI or soft mist inhaler is usually the lower-carbon choice.
Get technique right first
The best device is the one the patient can use effectively. Assess technique at every opportunity. A perfectly "green" inhaler used badly is still bad treatment.
Return used inhalers
Encourage patients to return used or unwanted inhalers to a community pharmacy for safe disposal (NG245 recommendation). Pharmacies have a contractual obligation under the NHS Community Pharmacy Contractual Framework to accept unwanted medicines returned by households (Community Pharmacy England).
How to switch inhalers safely
- Focus on the right medication and the right device for each individual — through shared decision-making with the patient and their family or carers, in line with NICE NG197.
- Assess and optimise inhaler technique at every opportunity.
- Prescribe by brand to ensure device continuity.
- Follow the patient up at 8–12 weeks to check device suitability and disease control (NG245).
- Do not undertake blanket switching of device or medication — this is explicit national advice, not just good manners.
💡 Trainee-friendly QIP starters aligned to NG245
Greener Practice and the NHS both have ready-made, guideline-aligned QIP templates that map directly to ARCP evidence requirements:
Non-Clinical Carbon — The Other 40%
Roughly 40% of a practice's carbon footprint comes from non-clinical areas such as buildings, travel and waste. The other 60% is dominated by prescribing (RCGP, 2025). Non-clinical areas are often led by managers rather than clinicians, but trainees can contribute — especially through QIPs and leadership activities.
Every practice is different. The most useful first step is to measure — use a free carbon footprint tool like SEE Sustainability or GP Carbon — and let the data tell you where to start.

The Green Impact for Health Toolkit offers a large menu of small projects a practice can do. Each one links to UN Sustainable Development Goals, and practices earn bronze, silver or gold awards (up to carbon-level) as they go.
🚗 Travel — staff and patients
The travel mix varies enormously. In poorer urban practices, better-paid staff often commute from outside the area — so staff travel is often a bigger emitter than patient travel.
COVID changed everything overnight, cutting face-to-face consultations and enabling more home-working. Some changes have since been reversed. Changing travel habits is slow — it requires understanding why people travel, and finding solutions that work for everyone.
As employers, practices can offer the cycle-to-work scheme to salaried staff (not partners). Local authorities, ICBs and health boards often run additional support. Practices leading on sustainability, like Frome Medical Practice, offer good examples worth looking at.
🏠 Buildings and energy
A meaningful proportion of UK GP estate sits in areas at risk of flooding. Before any major refurbishment, check whether the building is in the right place to keep delivering care long-term under a changing climate. Use the Environment Agency flood-risk service (England) or the equivalent service in your devolved nation.
Most of a building's carbon footprint comes from heating, heat loss and electricity. A carbon calculator tells you what to fix first (GP Carbon).
Classic moves: sensible temperature settings, timing of heating, improved insulation, then switching from gas heating to air-source heat pumps. More context at Energy Saving Trust.
Some surgeries will be able to install solar PV or even a wind turbine — but check the legal and mortgage position first.
♻️ Waste
The classic waste hierarchy applies: reduce, reuse, then recycle. Recycle is the last step, not the first. Greener Practice's waste management resource has practical examples.
Co-Benefits — Where Good Medicine and Good for the Planet Are the Same Thing
Co-benefits are interventions that simultaneously improve health and reduce environmental harm. These are the easiest things to recommend — because you are not asking a patient to sacrifice anything, you are offering them a double win.

🥗 Diet
Diet is one of the biggest drivers of non-communicable disease. High sodium intake, processed foods, red and processed meat increase risks of cardiovascular disease, some cancers and type 2 diabetes (Lancet, 2019; Bowel Cancer UK).

The EAT-Lancet Commission is not telling everyone to become vegan. It is suggesting a planetary health diet — mostly plants, with moderate meat and dairy — that benefits both people and planet.

⚠️ The hidden harms of intensive farming
- Antibiotics used as growth promoters feed into antimicrobial resistance.
- Farm effluent damages rivers and ecosystems (Guardian, 2022).
- Methane from cattle is a powerful greenhouse gas.
More on agriculture and biodiversity: WHO biodiversity guidance.
🚲 Active travel
The evidence for physical activity is enormous. If exercise were a drug, we would prescribe it for everything. The NHS recommends 150 minutes of activity spread through the week (NHS).
Activity is most sustainable when it is built into daily life, not bolted on. Swap part of a drive for a walk. Cycle part of the commute. E-bikes make this possible for many patients who thought cycling was beyond them. Some local authorities run borrowing schemes so people can try before they buy.

🚴 Practical resources
- Adapted bikes and trikes for people with disabilities: Cyclescheme.
- Cycle-to-work scheme (NB: available to salaried staff but not to GP partners): gov.uk guidance.
- Walking or cycling also reduces a patient's air pollution exposure compared with sitting in traffic.
🌳 Engaging with nature
Green front gardens have been shown to reduce stress (University of Sheffield), and urban green spaces improve wellbeing at population level (further research). Most contact with nature also involves movement, so the benefits stack.
Inequality, Health and Justice
The people who have done least to cause climate change are the people who suffer its harm most. This is true between countries (low-income nations suffer the worst effects of heatwaves, floods and food insecurity) and within countries (poorer neighbourhoods face the worst air, the damplest housing and the fewest green spaces).

📖 Tudor Hart's Inverse Care Law
Tudor Hart captured it in a single famous line: good medical care tends to be least available where it is most needed — and this distortion is worst where healthcare is most exposed to market forces.
Paraphrased from Julian Tudor Hart, The Lancet, 1971 — still true today.
For GPs, the point is practical. Wherever possible, we should:
- Actively seek out and serve the patients who need us most — rather than the ones who find us easiest.
- Ask about housing, fuel poverty and air quality as part of the history, especially in long-term conditions.
- Build links with local social prescribing, community groups and advocacy services.
- Think before complaining about "frequent attenders" — they are usually the people the system is failing, not gaming.
More on health inequalities and climate from Greener Practice.
Population, Justice and Women's Health
There is a body of opinion (Population Matters, and supporters including Sir David Attenborough) arguing that population is a key factor in the planetary health crisis. More people means more food, water and energy needed, and more waste produced.
At the same time, this is a sensitive area — because of justice.

📊 The inequality problem with "population" as a solution
Oxfam's most recent carbon inequality analysis shows that the richest 1% of the world's population (around 77 million people) were responsible for about 16% of global CO₂ emissions, while the poorest half of humanity (3.9 billion people) were responsible for around 8% (Oxfam, 2025). Yet the largest families are generally in the poorest countries — where individual emissions are lowest. Framing "population control" as the answer therefore risks putting the responsibility onto the people least responsible for the crisis.
Planned family sizes are genuinely in the interests of both planet and patients. The appropriate role for UK primary care is clear and patient-centred:
- Offer the full range of contraception and women's health services.
- Make these services easy to access and culturally sensitive.
- Keep the patient's interests at the centre — never someone else's political agenda.
🧭 A useful principle
"What matters to this patient?" is always the right starting point. Policy conversations about population belong in society, not in the consulting room.
Voices from the Field — Wisdom from Trainees, Trainers & Community Forums
Guidelines tell you what to do. Colleagues tell you how it really feels to do it. This section pulls together practical wisdom from the Greener Practice Trainee Forum (now more than 200 UK GP trainees), the Centre for Sustainable Healthcare networks, published accounts from GP registrars working on sustainability, Greater Manchester Greener Practice educational videos, and podcast interviews with GP sustainability leads.
Every tip below has been checked against RCGP, NICE, BNF and GMC guidance. Nothing that conflicts with official advice has been included. Nothing that touches UK law has been included in a way that goes against it.
🧭 How to read this section
Think of this as the conversation you would have with a registrar who has already done their sustainability QIP — the honest version, after the write-up was submitted. It is not a second set of guidelines. It is the lived experience behind them.
🗺️ The pattern map — what trainees keep saying
Five themes appear again and again across the forums, blogs and videos. They show up in every practice size, in every deanery, and in every ST year.
Start small, start clinical
Trainees who finish their sustainability QIP say the same thing: "we began with something we were already doing." Inhaler reviews, overdue medication reviews, SABA overusers — these are clinical tasks that already need doing. Adding a carbon lens costs no extra time.
Bring the team before the bin
Projects that focus on bins and energy first often stall. Projects that start with a staff conversation about why sustainability matters tend to succeed. Hearts before waste streams.
Frame the gain, not the loss
Partners respond much better to "better asthma control, fewer admissions" than to "lower carbon footprint". The carbon benefit is a bonus, not the headline. This is reported in Greener Practice's own accounts and by the NW Canada GP study on barriers.
Guidelines help, not hinder
A Lancet Planetary Health systematic review of physicians' views identified clear guidelines from respected bodies as the single biggest facilitator. When the RCGP, NICE and local ICB speak with one voice, change happens. Cite them early in your proposal.
Co-benefits are the secret weapon
Every experienced sustainability lead says the same: lead with the human benefit. Active travel, plant-rich diets, social prescribing — each helps a patient in front of you, and also helps the planet. Talk about the patient benefit. The carbon follows.
✅ What actually works — a trainee-to-trainee summary
These are the specific, concrete moves that forum members credit with making their projects succeed. None of them contradict RCGP, NICE, BNF or GMC guidance. All of them are safely within the scope of GP training.
| Situation | What trainees say works | Why it works |
|---|---|---|
| Picking a QIP topic | Use the Greener Practice or SusQI project library — ready-made protocols, measures and templates. | Saves weeks of design time. Already aligned with Greener NHS measures, so your data is credible. |
| Getting the partners on board | Show your practice's position on the OpenPrescribing greener NHS measures before the meeting. | Data beats opinion. Seeing their own practice ranked in the region changes the conversation. |
| Reviewing asthma patients | Start with SABA-only asthma patients — a group NICE NG245 (2024) now explicitly wants reviewed onto ICS/formoterol AIR or MART. | You are not "changing practice for carbon". You are doing a high-value clinical review. Carbon reduction is a side effect. |
| Switching inhaler devices | Always shared decision-making. Never blanket switching. Always follow-up technique. | This is explicit national advice. Blanket switching erodes trust and harms control. |
| Deprescribing | Start with anticholinergic burden reviews in frail/elderly patients. | NICE and RCGP both endorse it. Carbon reduction follows quietly. A clinical win. |
| Building team buy-in | Run one short "lunch and learn" session with a Greener Practice two-minute video. | Short, visual, credible. Staff remember "why" rather than being handed "what". |
| Evidencing in the ePortfolio | Name it. Use language like "sustainable clinical practice" and "four principles". | Planetary health WPBA evidence is often already there — it just needs labelling. |
| Communicating with patients | Mention the co-benefit only if the patient opens the door first. Otherwise lead with health. | Most patients engage warmly when asked; a few resent it being raised. Let the patient set the pace. |
💬 Consultation phrases that trainees say actually land
These are phrasings reported repeatedly by trainees and educators in the Greener Practice network, Copernicus/RCGP sustainability course materials, and the Greater Manchester educational videos. They have been rewritten to sit comfortably alongside standard UK GP shared decision-making language.
🌬️ Starting an inhaler conversation
- "I'd like us to look at your inhalers together — partly because we want your asthma working as well as it can, and partly because there are newer options that are kinder to the environment."
- "Your reliever inhaler tells us how controlled your asthma really is. Can we look at what a better plan might look like for you?"
- "There's more than one type of inhaler. Some are easier to use, some have a smaller environmental footprint. Let me explain the options and see what fits for you."
💊 Gentle deprescribing language
- "Some of these tablets were started a long time ago. Can we check together whether they are still doing what we wanted them to do?"
- "Sometimes the simplest improvement is fewer tablets rather than more."
- "What matters most to you about the way you take your medication?"
🌳 Opening a social or green prescribing door
- "Alongside medication, there's good evidence that time in green space helps with mood. Would that be something you'd be open to trying?"
- "There's a walking group / community garden / parkrun near here. I can get you the details if it would be useful."
- "Our social prescriber could speak to you about things that might help — no tablet involved. Would you like me to refer you?"
💨 Taking a pollution history
- "Is your home easy to heat and dry, or is there any damp or mould?"
- "Do you live near a busy road, or is there a lot of traffic where you walk?"
- "Do you use anything indoors that makes smoke — a log burner, gas cooker, candles?"
📊 The hierarchy of effort — where to put your energy
A repeated theme across the Greener Practice network and the Centre for Sustainable Healthcare's teaching is that not all sustainability actions are equal. Some save a lot of carbon for a little effort. Others are the other way around. Trainees ask the same question: "where should I start?" The answer below is a synthesis of forum wisdom, not a single source.
⚠️ The "bin trap"
The most common trap described by trainees is starting their sustainability journey at the bottom of this pyramid. Recycling and bins feel visible and satisfying. But waste disposal is about 0.5% of the primary care footprint. A single well-run medication review saves more carbon than a year of better bin discipline — and helps a patient directly.
🌟 Trainee-to-trainee wisdom
The observations below are drawn from published accounts by GP trainees and registrars working on sustainability — including Dr James Pumphrey's account of working with his trainer Dr Abigail Fry on a sustainable QIP, Dr Jawad Haq and Dr Vik Puri's RCGP blog on their Greener Practice initiative as ST3s, and Dr Vasu Siva's inhaler prescribing project. All statements have been summarised and rewritten — no direct quotation.
🩺 "The project felt different to my other QIPs"
Trainees consistently describe their sustainability QIP as one of the more meaningful pieces of ePortfolio work they did — partly because the outcome felt like it mattered beyond the tick-box. Dr Pumphrey's reflection captures this: a sense that the clinical and the environmental were not really two separate things.
📊 "Measure first, move second"
The accounts that describe successful practice-level change start with measurement. The GP Carbon Calculator and SEE Sustainability were both used by registrars to show colleagues where the big carbon was sitting — before proposing what to change.
🧑⚕️ "We engaged the whole team, not just the clinicians"
Dr Siva's account emphasises engaging receptionists, pharmacists and managers — not just GPs. People were "shocked" when they saw the equivalent mileage of a single MDI inhaler. The visual comparison did the work that statistics alone never did.
🌍 "Start with what you're already doing"
Drs Haq and Puri describe beginning as ST3s by using the free Green Impact for Health toolkit — they point out how many of its actions the practice was already doing without labelling them as sustainability. Half the work was naming what already existed.
📺 Insights from UK planetary health videos and podcasts
Below is a synthesis of teaching points drawn from content by UK planetary health educators whose work is directly aimed at primary care or consistent with UK guidelines — selected for alignment with RCGP, NICE and GMC guidance. Sources include Greener Practice educational videos, the RCGP–Greener Practice–Copernicus sustainable healthcare course, the Greater Manchester greener inhaler prescribing videos by Dr Mike Poplawski, the YORLMC podcasts, and the UKHACC "Environmentally Sustainable Primary Care" book launch content.
🎬 Dr Aarti Bansal (Greener Practice co-founder) — the communication principle
The core teaching point: most patients engage warmly when the climate and health link is raised gently. The reluctance is usually ours, not theirs. The recommended approach is to connect it to what the patient is already there to discuss — physical activity and diet with cardiovascular patients, air pollution and climate-friendlier inhalers with respiratory patients, green space with people with low mood.
Why it matters: links directly to RCGP's "what matters to you" model and to NICE NG197 on shared decision-making. Nothing here contradicts official guidance.
🎬 Dr Terry Kemple (former RCGP National Sustainability Lead) — the small steps principle
The core teaching point: every small positive change brings benefits, and the sooner everyone starts the larger the combined impact. Waiting for perfect guidance, perfect funding or perfect leadership from above is a common reason sustainability projects never start.
Practical translation: do not wait for your next CPD cycle, your next ARCP, or your new job to begin. Start with one patient, one inhaler review, one deprescribing conversation this week.
🎬 Dr Mike Poplawski (Salford GP) — the visual comparison technique
The core teaching point from his educational videos: use concrete visual comparisons patients can picture. Greener Practice widely-cited figures indicate that a typical salbutamol pMDI has a carbon footprint roughly equivalent to driving around 175 miles in a small car, while the DPI equivalent is under 1 kg CO₂e. The exact numbers vary by brand and inhaler type, but the order-of-magnitude difference is consistent. Patients and staff remember images — "175 miles" sticks, "28 kg CO₂-equivalent" does not.
Use this in patient conversations and staff teaching alike. But note: always lead with the clinical reason first (better technique, fewer exacerbations). The carbon comparison is a supporting argument, not the opening one.
🎬 Sustainable healthcare teaching — a practical four-question approach
Across the RCGP–Greener Practice–Copernicus sustainable healthcare course materials and other UK teaching resources, the RCGP's four principles of sustainable clinical practice are commonly translated into four practical questions for everyday clinical decisions:
- Is it needed? — prevention and avoiding overdiagnosis.
- Does the patient understand and own it? — empowerment, shared decision-making.
- Is the pathway lean? — no duplication, no unnecessary follow-ups.
- Is there a lower-carbon option? — only after the first three are answered.
This is a simple, memorable way to bring the four principles into a normal UK consultation. It is consistent with RCGP, NICE and GMC guidance.
🎬 UKHACC & Environmentally Sustainable Primary Care — the trust principle
The core teaching point: primary care clinicians are consistently among the most trusted professional groups in the UK (a pattern seen year after year in the Ipsos Veracity Index). That trust is not a small thing. When GPs explain the link between climate, health and clinical care, patients listen in a way they do not listen to politicians or campaigners. Using that credibility carefully and in proportion is a professional responsibility.
The counterpoint, also acknowledged: that trust is damaged if patients feel lectured or made to feel guilty. Lead with their health. Let the planetary link arrive naturally.
🚫 What forums consistently advise against
These are recurring warnings from trainees, trainers and Greener Practice leads. Each one is consistent with UK law, RCGP curriculum guidance, and GMC Good Medical Practice.
⛔ Don't do these
- Do not blanket-switch inhalers — explicit national advice, not just a forum opinion.
- Do not lecture patients about climate. Raise it when it fits; drop it when it doesn't.
- Do not chase prescribing numbers over individual patient care — outcomes lead, carbon follows.
- Do not use patient-identifiable data on social media, even for good sustainability causes. Applies just as strongly here as anywhere else.
- Do not present personal activism as practice policy — the GMC boundaries around personal and professional voice still apply.
✅ Do these instead
- Switch with shared decision-making, one patient at a time.
- Raise climate only in contexts where it is clinically relevant.
- Use data and outcomes to make the case for change.
- Follow normal practice information-governance rules for QIPs.
- Use your own non-work channels for activism — and know the GMC position on peaceful climate action.
📖 Legal & professional context
In April 2024, the directors of Greener Practice wrote publicly to the GMC about the regulator's approach to doctors taking part in peaceful climate action. This is a live area. If you are considering any form of public activism, separate it clearly from your clinical role, check the latest GMC position, and talk to your defence organisation (MDU/MPS/MDDUS) for personal advice. Nothing on this page constitutes legal advice.
🎯 Pulling the threads together
The community's synthesis — 8 lessons you won't find in the guidelines
- The best planetary health project is usually a good clinical project with a sustainability lens added.
- Measure before you change. GP Carbon, SEE Sustainability and OpenPrescribing are free and credible.
- Start with people, not bins. Culture change beats infrastructure change every time.
- Frame gains, not sacrifices. "Better asthma control" lands; "lower carbon" does not — until later.
- Shared decision-making is the single most important clinical skill for this work. Everything good flows from it.
- Co-benefits are the honest easy wins — active travel, plant-rich diet, social prescribing, green space.
- Label what you already do. Your ePortfolio is full of planetary health evidence that is not currently named.
- Follow the rules — RCGP, NICE, BNF, GMC. No sustainability action is worth a safety or probity compromise.
What You Can Do Tomorrow
Big subjects can feel overwhelming. Here are concrete things a trainee can do in the next week — no permission or extra time needed.
🩺 In the consulting room
- Ask the "two questions" in every consultation today.
- Identify patients on SABA-only regimens and review them against NG245 (2024) — most should move to ICS/formoterol AIR or MART.
- Think about lower-carbon inhalers when starting or switching — but never blanket switch.
- Offer social, green or blue prescribing instead of a drug, where evidence supports it.
- Take a pollution and housing history in respiratory and cardiovascular consultations.
📋 For your portfolio
- Write one reflective log entry on a planetary health consultation.
- Pick a Greener Practice QIP and get it signed off with your trainer.
- Run a simple prescribing audit (DPI vs pMDI, anticholinergic burden, repeat review backlog).
- Do a CbD where sustainability is part of the discussion.
- Look up your practice's position on the Greener NHS inhaler measures via OpenPrescribing.
🏢 At practice level
- Suggest a practice carbon footprint audit with GP Carbon or SEE Sustainability.
- Start or join a Green Impact for Health project.
- Help set up an inhaler-return bin in your practice or local pharmacy.
- Raise sustainability in a practice meeting — ask one good question.
🙋 For yourself
- Listen to the YORLMC podcasts on your next commute.
- Try the Clean Air Hub calculator.
- Swap one short drive this week for a walk or cycle.
- Notice how much of planetary health is simply good medicine.
Evidencing Planetary Health in WPBA
Planetary health is now explicitly recognised across many WPBA capabilities. The RCGP guidance on Planetary Health & Sustainability in WPBA is the canonical source — here are some practical ideas you can log on FourteenFish ePortfolio.
| WPBA tool | Planetary health angle | Example |
|---|---|---|
| CbD | Discuss sustainability implications of prescribing choices and social prescribing. | CbD on a polypharmacy review where a deprescribing decision also reduced carbon. |
| COT | Consider the patient's air quality exposure and home environment in your data gathering. | COT on a patient with recurrent chest infections — history includes log burner use at home. |
| Shared management planning | Shared planning reduces unnecessary prescriptions, investigations and procedures. | Evidence your shared decision-making around inhaler choice. |
| Leadership activity | Lead a practice project with a sustainability focus. | Practice energy audit, waste stream review, bin compliance review, anticholinergic burden project. |
| Prescribing assessment & Clinical Case Review (CCR) | Reflect on sustainable prescribing patterns. | Review of DPI vs pMDI prescribing across your own patients. |
| QIA / QIP | Many Greener Practice QIPs are trainee-friendly and strong ARCP evidence. | Moving SABA-only patients onto NG245-concordant AIR/MART; inhaler recycling pathway; deprescribing project. |
| Learning log | Reflective entries on consultations where planetary health shaped your decision. | A reflection on avoiding a low-value investigation after an ICE-focused consultation. |
💡 Trainee tip
Planetary health evidence is often already there in your everyday consultations. You are choosing DPIs, you are deprescribing, you are exploring ICE, you are doing shared decision-making. The trick is to name it. A line in your reflection like "This also represented sustainable clinical practice — the device switch lowered emissions and improved technique" turns ordinary evidence into explicit planetary health evidence.
For Trainers and TPDs
Planetary health is a topic many trainees arrive knowing a bit about, caring a lot about, but feeling unsure how to apply. Your job is less to teach them facts and more to help them use what they already know in clinical reasoning.
🧭 Tutorial framing ideas
- Start with Dr Ram's two questions — role-play applying them to a real case.
- Take one of the trainee's recent consultations and re-examine it through the four principles.
- Debate: is a patient with uncontrolled asthma "allowed" to stay on a pMDI?
🤔 Reflective prompts
- "What did you prescribe today that the patient didn't really need?"
- "Where in this consultation could you have used social or green prescribing?"
- "Who in your list today is most affected by fuel poverty, mould or air pollution?"
🧪 Useful scenarios
- A 34-year-old asking for a sick note for work after a heatwave shift.
- A 6-year-old with worsening asthma living near a ring road.
- A 70-year-old on 14 repeat medications, confused about what they are all for.
- A newly qualified colleague wanting to do "something green" for their QIP.
⚠️ Common trainee blind spots
- Seeing planetary health as "extra" rather than integral to good medicine.
- Thinking it is all about recycling and bins.
- Missing the justice angle — assuming it is about individual lifestyle alone.
- Blanket-switching inhalers without shared decision-making.
- Forgetting to log planetary health evidence they are already generating.
🎯 TPDs — half-day release ideas
- Patient actor session: consultation with a mum asking to switch her child's inhaler for environmental reasons.
- Small-group exercise: each group takes a common presentation and maps the two questions + four principles.
- Invite a local Greener Practice lead to run a session.
- QIP workshop using the Greener Practice project library.
FAQ
Is this really my job, or is it for the government and NHS leaders?
Both. System change is essential, but around 60% of general practice's carbon footprint is associated with prescribing (RCGP, 2025). GPs are uniquely placed because we hold the prescribing pen for most of primary care.
Do I have to push every patient onto a DPI?
No. The first priority is always good disease control and a regimen that is concordant with NG245 (2024). Blanket switching is explicitly not recommended. The aim is shared decision-making, good inhaler technique, and — where it fits the clinical need and the patient can use it well — choosing the device with the lowest environmental impact, which will often be a DPI or soft mist inhaler.
Isn't individual action pointless compared with big industry?
Two things at once. Individual action matters, because in primary care the individual clinician is the system at the point of prescribing. And advocacy matters — GPs have a long, credible history of shaping policy on smoking, alcohol and road safety. The same is possible for planetary health.
How do I bring this up with an older partner who is sceptical?
Lead with patient benefit. Framing a move to NG245-concordant AIR/MART regimens as "better asthma control, fewer exacerbations, alignment with national guidance" lands much better than "lower carbon". Frame Green Impact as "awards and a nicer practice" rather than virtue. Many sceptical colleagues come around once they see the clinical case.
What if my practice does nothing at all about sustainability?
You can still do a lot. Your own prescribing is yours. A trainee-led QIP is a great way to start without needing partner buy-in. Pair up with your practice pharmacist — they often have the data and the appetite.
What do IMGs find most confusing about UK planetary health language?
Usually three things: shared decision-making (different from informed consent), social prescribing (no pills involved), and the UK-specific polypharmacy culture. Spending tutorial time on these three topics pays off more than memorising inhaler brand names.
What if a patient doesn't want a "greener" option?
Respect their choice. Shared decision-making works both ways. Your job is to offer information and options — not to impose an agenda. Prescribing something the patient will not use is bad care and bad for the planet.
🎯 Final Take-Home Points
- Planetary health is in the RCGP curriculum now. It is assessable, it is relevant, and it is not going away.
- Most of it is just good medicine. Prevention, empowerment, lean pathways and low-carbon alternatives are the four principles — every good GP already leans on them.
- Two questions change the consultation. How does the environment affect this patient? How does my management affect the environment?
- Medication is the biggest lever. Overdiagnosis and polypharmacy are planetary health problems as much as clinical ones.
- Inhalers are the single biggest quick win. Optimise disease control first, then device — but never blanket-switch.
- Co-benefits are your best friend. Active travel, plant-rich diets, social prescribing — each is a double win.
- Justice is central. Those least responsible for environmental harm suffer most from it. Tudor Hart's inverse care law still applies.
- Air pollution is a medical emergency. Up to 38,000 UK deaths a year are attributable to air pollution (UKHSA). Take a pollution history.
- Log what you already do. Your FourteenFish ePortfolio is full of planetary health evidence you haven't labelled yet.
- Start small, start tomorrow. One consultation. One audit. One conversation. The planet is big — the next step isn't.
This is a really helpful and comprehensive look at Planetary Health and should be required reading for all trainees AND trainers!
I didn;t realise how much our activites as dcctors could affect the planet before now