MRCGP & GP Training
Learning Log Entries Made Easy
DOWNLOADS
path: LEARNING LOG ENTRIES
What is a Learning Log Entry (LLE)
A Learning Log is a journal which evidences your own learning and skills development in your ePortfolio. The current RCGP’s e-Portfolio has been developed by a company called FourteenFish. The ePortfolio is not just a diary or record of “What you have done” during GP training, but a record of what you have learned, tried and critically reflected upon. It is a personal record of your own learning. As such it is a document which is unique to you and cannot be ‘right’ or ‘wrong’. A Learning Log helps you to record, structure, think about, reflect upon, plan, develop and evidence your own learning
For example, if in your Learning Log you include details of what you did or how you did something then consider asking yourself questions such as:
- Did it go well? Why? What did you learn?
- Did it go badly? Why? What did you learn?
- How can you improve for next time? What might you try the next time?
A Learning Log contains your record of your experiences, thoughts, feelings and reflections. One of the most important things it contains is your conclusions about how what you have learnt is relevant to you and how you will use the new information / knowledge / skill / technique in the future.
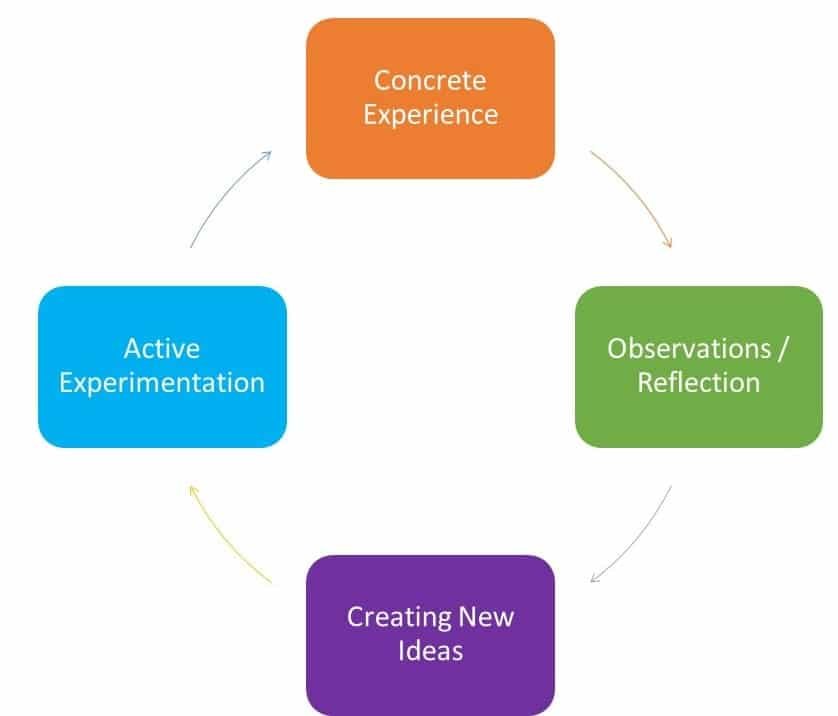
This is Kolb’s LEARNING CYCLE. It’s illustrates the process of how we learn from a situation or experience. Some people call it the EXPERIENTIAL learning cycle. Can you see how you might use it to write up your learning log entry? Look at the 3 questions on the left – where do they fit in with the cycle?
But why do I have to write Learning Logs? I've enough on my plate!
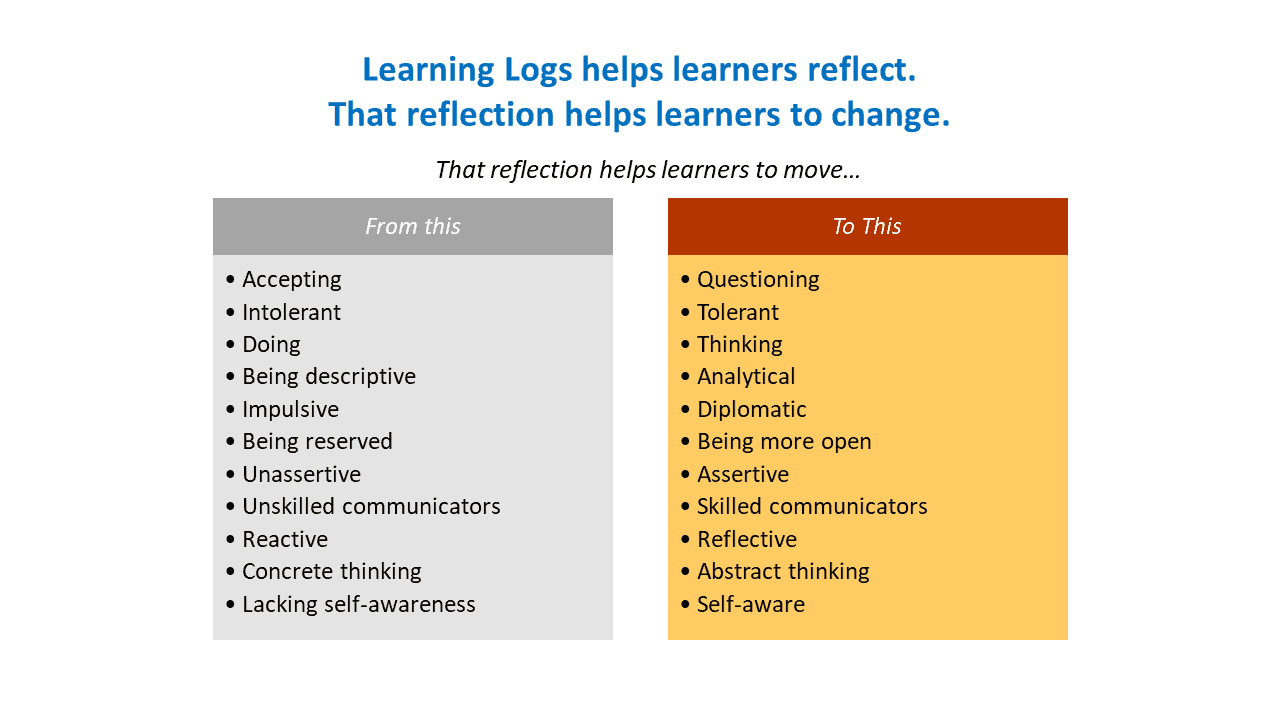
Research has identified that reflection can help people to change. Some of the changes which have been identified are listed in the infographic on the left.
These entries will contribute to the evidence that your educational supervisor will consider at your 6 monthly educational supervision meetings. Log entries can contribute to your evidence in two ways. They determine your curriculum coverage and contribute to the evidence in the 13 competency areas if they are ‘validated’.
Maintaining your log is therefore just as important as completing your formal assessments.
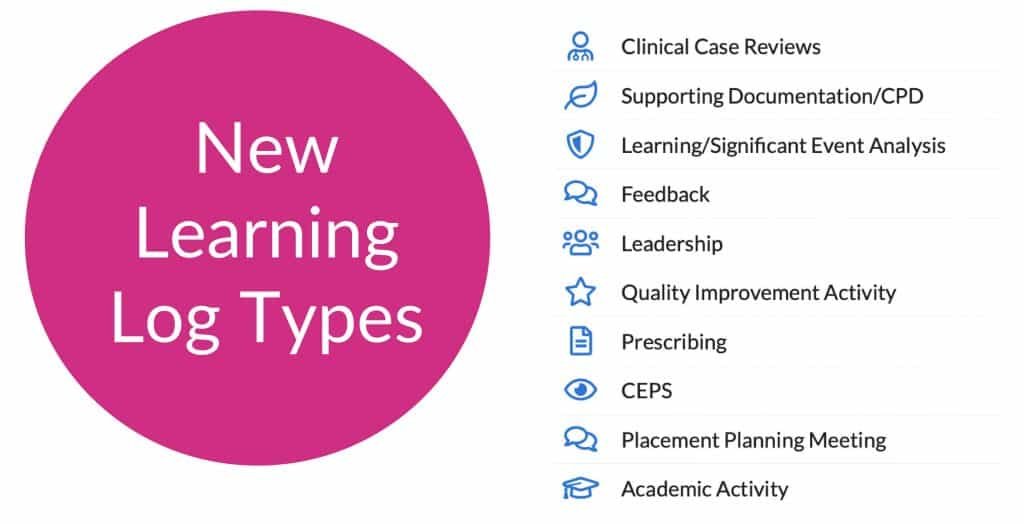
Types of Learning Log Entries
Learning log entries should cover the full range of learning opportunities and cover both the competencies AND the whole curriculum over your 3 years in training. Document interesting cases, tutorials, educational events, online learning, significant event analyses, audit, presentations, out-of-hours sessions and what you have done on the GP scheme’s half-day release programme.
Include things like…
- What you found easy / difficult.
- What you enjoyed / disliked.
- What problems you need to work on next / how you are progressing.
- How you feel about things – the situation, the course, the tutorial etc
- You can include information from your life as a whole, but the focus should be on how this is affecting your learning.
- You should aim to analyse and reflect, not just to describe. Your journal should answer questions like
‘Why…?’ and ‘How…?’, not just ‘What…?’ and ‘When…?’
ePORTFOLIO LEARNING LOG CATEGORIES
TYPES OF THINGS YOU CAN WRITE ABOUT

ePORTFOLIO LEARNING LOG CATEGORIES
I get confused between the Curriculum, Capabilties & Clinical Experience Groups
We understand the confusion – they both start with a C and they are all educational terms. But they mean totally different things.
- The Curriculum in simple terms is basically the set of subjects that make up a course of study in a school or college. In other words, they are all the topics you are meant to know about during your GP training programme; the curriculum defines the knowledge, skills and attitudes associated with each topic. An independent GP has to have some knowledge and skills and develop certain attitudes. The curriculum will help you identify what is what.
- The Clinical Experience Groups (CEG) are patients who are grouped together by a specific commonality. For example, the group “Infants, Children & Young People” – the commonality here is age – i.e. anyone under the age 19. (Although on a personal note, I strongly believe that Young People (14-18) should not be grouped together with Infants and Children – the needs are VERY different. I and many others think it is wrong to homogenise them!). Anyway, back to the Clinical Experience Groups – in the old MRCGP you had to demonstrate that you had enough experience in most of the GP curriculum. But as you can imagine, that curriculum consisted of so many items that GP trainees often went into panic mode and tried to write about log entries just to map them to the curriculum to show that they had experience in most areas. This resulted in the Learning Log Entries becoming a tick box exercise than a reflective and learning one. So, to move away from this, trainees now how to map to Clinical Experience Groups and NOT the GP curriculum. There are only 9 or so CEG categories – enabling the trainee to easily provide evidence of learning in all 9 areas. This then helps the trainee concentrate on the reflection and learning and moves them away from a numbers ticking exercise. Besides, all of us educators know that it is almost impossible to cover the whole of the contents of the GP curriculum in a 3 year programme and in fact, the GP curriculum was developed to aid lifelong learning in General Practice.
- Capabilities are abilities or attributes, described in terms of behaviour, key to effective performance within a particular job. They provide a common language for describing performance and the abilities/attributes displayed by individuals. Currently the RCGP defines 13 competencies. Put another way, everything any competent GP does can be mapped out into one or more of these 13 broad areas (competencies). Therefore, if by the end of training a trainee can demonstrate that they are good (i.e. competent) at all 13 areas, then it makes logical sense that they are also competent at being an independent GP.
THE CLINICAL EXPERIENCE GROUPS
- Infants, children and young people [under the age of 19yrs]
- Gender, reproductive and sexual health (including women’s, men’s, LGBTQ, gynaecology and breast)
- People with long-term conditions including cancer, multi-morbidity and disability
- Older adults including frailty and/or people at end of life
- Mental health (including addiction, alcohol and substance misuse)
- Urgent and unscheduled care
- People with health disadvantage and vulnerabilities (including veterans, mental capacity difficulties, safeguarding and those with communication difficulties/disability)
- Population Health and health promotion (including people with non-acute and/or non-chronic health problems)
- Clinical problems not linked to a specific clinical experience group
WPBA PROFESSIONAL CAPABILITIES
The framework for WPBA comprises 13 competences and these are assessed throughout the three years using different tools to demonstrate evidence of competency. Your need to pick situations to write about as learning log entries which demonstrate several of these competences.
- Communication and consultation skills (CS)
- Practising holistically, Promoting Health & Safeguarding (PH)
- Data gathering and interpretation (DG)
- Making a diagnosis/decisions (MD)
- Clinical management (CM)
- Managing medical complexity & Promoting Health (MMC)
- Organisation, Management & Leadership (OML)
- Working with colleagues and in teams (WWC)
- Community orientation (CO)
- Maintaining performance, learning and teaching (PLT)
- Maintaining an ethical approach (Eth)
- Fitness to practise (FTP)
- Clinical Examination & Procedural Skills (CEPS)
How can I ensure I get validated for a capability?
The Professional Capabilties are the things you ultimately have to provide evidence for. However, only your clinical or educational supervisor can only validate log entries against the professional competences. And they will only do that if they are of sufficient quality to make a judgement about your level of progress with that competency. So, to help increase the chances of them validating something you have written to a competency…
- Familiarise yourself with the word pictures used to describe the criteria for assessing the 13 professional competency areas
- Make sure your log entry writes SPECIFICALLY about the competency you are aiming for.
- Make sure the quantity AND quality is there for that competency. Don’t just write a one-liner and think you will “get the mark”. You only get the mark if what you have written is deep and meaningful and that relates back to the ISCE criteria of reflection (click on the buttons above to read more about reflection).
- If there is insufficient quantity within the learning log then it is unlikely that an adequate grade will be given.
- If there is a lot of quantity but no quality, again it is unlikely that and adequate grade will be given.
Compare these two and tell me which you think is the better.
A Romanian man came in with pain in his right tooth and right cheek. He’d been to several doctors (including OOH) and essentially wanted antibiotics.
COMMUNICATION SKILLS
It was a difficult consultation for two major reasons:
1. Language barrier – speaks only Romanian and only “sprinkles” of English words.
2. Wanted antibiotics and has been told the previous day by OOH GP and on-call dentist that he doesn’t need antibiotics.
This was how I tackled the difficulties I encounters:
1. LANGUAGE BARRIER –I was very careful with my consultation skills. I made sure I didn’t use complicated words and kept the conversation simple. I kept checking he understood what I said. Clearly I must have communicated very well because he said “you’re the doctor, you know the best”.
2. WANTS ANTIBIOTICS – His agenda was to get antibiotics because he believed it was infected. He said the doctor and dentist he saw yesterday did not think it was infected and so I asked him why he came to me. He said he felt it was still infected and the other two had got it wrong. I also made sure he understood why I wasn’t giving the antibiotics – I explained he did not have a fever or pus and that my examination and all the observations I did were normal.
Can you see that in this first write up, yes there is something in there about COMMUNICATION SKILLS but the depth is just missing compared with write up number two. In number two, the person clearly understands exactly what he or she is doing and details this – but number 1 doesn’t. Number 1 just writes in vague terms like “I explained”. Number 2 uses words like validated him, his agenda and so on. And in terms of communication, number one says “I kept things simple” – which is good – but number 2 gives lots more examples of how he altered his communication styles and the methods he used.
A Romanian man came in with pain in his right tooth and right cheek. He’d been to several doctors (including OOH) and essentially wanted antibiotics.
COMMUNICATION SKILLS
It was a difficult consultation for two major reasons:
1. Language barrier – speaks only Romanian and only “sprinkles” of English words.
2. Wanted antibiotics and has been told the previous day by OOH GP and on-call dentist that he doesn’t need antibiotics.
This was how I tackled the difficulties I encounters:
1. LANGUAGE BARRIER – I used the google translate to communicate with him. I started from the process of connecting with him by greeting him, showing interest in his complains and telling him sorry for the pain he is feeling. He said no one ever used Google Translate for him and this was better. Although he couldn’t type fast, he used the “speech to text” app on his phone which translated what is spoke from Romanian to English text. I made sure I didn’t use any complex phraseology when using Google Translate to reduce the chance of losing meaning through translation.
2. WANTS ANTIBIOTICS – His agenda was to get antibiotics because he believed it was infected. He said the doctor and dentist he saw yesterday did not think it was infected and so I asked him why he felt it was infected. He said because it was very painful, and he had never experienced anything like this before. I validated him that in many cases, infection is painful but that this on its own is not a reliable indicator of infection. I went on to explain that this didn’t look infected because absence of other features: he did not have temperature, no pus, not feeling sick or poorly, eating and drinking and all his observations were normal. So, our discussion moved nicely from antibioics to what could be done to relieve the pain.
Try to write up your Log Entries on interesting things that you have discussed with others – for example, in debriefs, if you felt you were out of your depth, or just felt like you needed some guidance. That discussion will ‘open up’ your mind thus enabling you to write up a more meaningful entry that not only encourages you to summarise and therefore consolidate your learning but also helps you cover some Professional Competences well.
Is there a 'best' or 'correct' way of producing a Learning Log?
A good quality log entry is one that shows good reflection, which means that it demonstrates your insight into how you are performing and how you are learning from your everyday experiences. The log should be relevant to you and your job / studies / role / activities. There is no ‘right’ or ‘wrong’ way of producing a Learning Log. Perhaps the 3 key questions when engaging in the process of producing a Learning Log are:
- Am I being honest with myself?
- Is this a useful process for me?
- Is this helping my own process of learning?
If the answers are ‘yes’ then your Learning Log is correct and right for you. If the answers are ‘no’, then talk to your Trainer or Educational Supervisor about it so that they can help you find a way that works.
Learning cannot happen without reflection. And reflection is a skill that you can be taught and that you can build upon.
A good learning log will:
Be written in a personal style, using the first person singular (I).
Analyse and comment, not just describe.
Focus on learning.
Make connections between ideas.
Show links between entries from day to day.
Show evidence of planning.
Show evidence of looking back.
Show evidence that you are reflecting on your progress.
A good learning log will show:
- Some evidence of critical thinking and analysis, describing your own thought processes;
- Some self-awareness demonstrating openness and honesty about performance along with some consideration of your own feelings;
- Some evidence of learning, appropriately describing what needs to be learned, why and how.
By the way, did you know that human psychology tells us that most of the time our brains don’t like to think – it’s too exhausting. Our brain likes patterns that it recognises and it loves familiar stuff because it doesn’t find that sort of work too taxing.
However, it does find thinking, analysis and reflection taxing! And it gets exhausted from doing so. If you have ever felt like this after some log entries, it’s probably because you are reflecting and analysing (hurray!!!). You might not like this feeling (because it is tiring) but you can say something positive to yourself to get your motivation levels back up, like “I know I’m finding this quite taxing, but that means I am learning and becoming a better me!”. But if you find entering a learning log as mundane and boring and can’t wait for it to be over, then your entry is likely to descriptive and the value to you OR OTHERS will be zero because it will be devoid of learning.
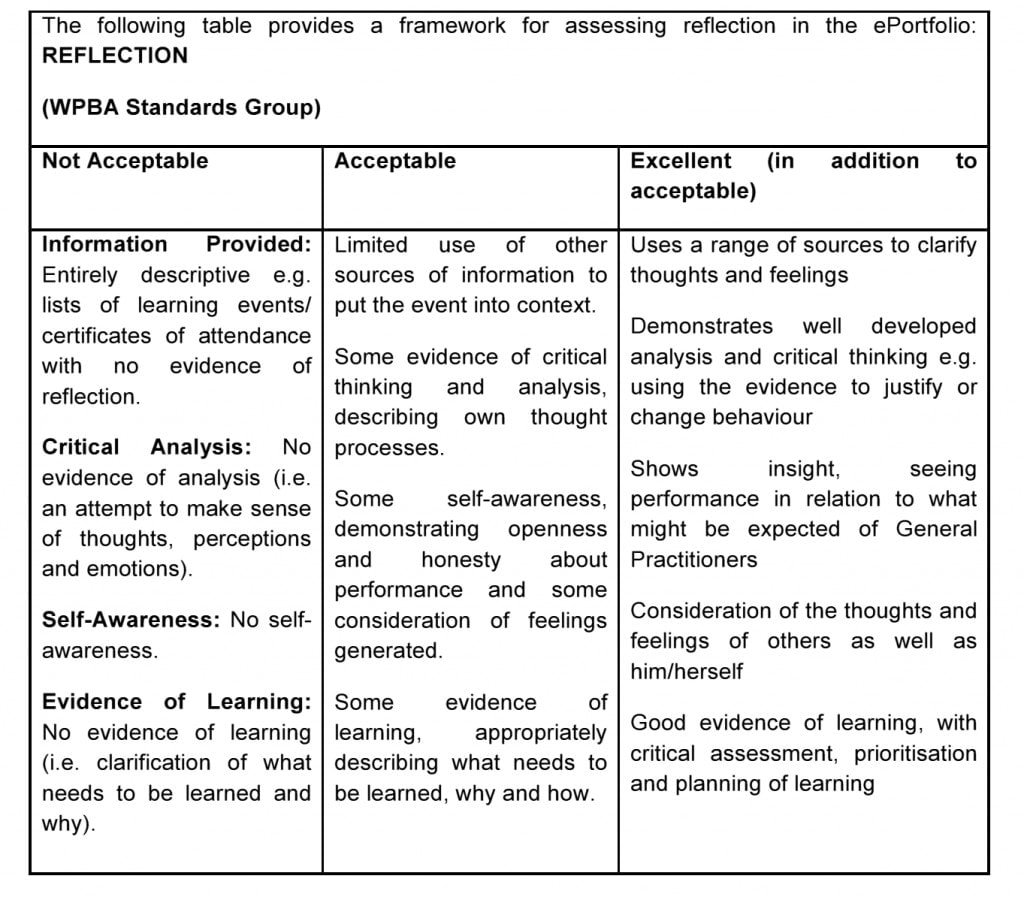
What is a good entry and what is not... according to the RCGP?
The Dr Bawa-Garba Case
The Dr Bawa-Garba case has produced disquiet amongst trainees because evidence from a professional conversation, recorded on a reflective-style proforma, albeit not from her ePortfolio, fed into the hospital investigation and trial. This website does not explore the completion of proforma being used outside an e-portfolio. Rather our focus here is on improving the quality of a personal LLE.
We would urge trainees who have concerns about the use of their log entries outside the remit of an ePortfolio, with their Training Programme Directors.
Top Tips on Learning Log Entries
- Just start writing, don’t aim for perfection.
No one is going to expect you to produce perfect log entries from Day One of your training programme. Your Supervisor will expect to see improvement in the quality of your log entries and more importantly, your insight, as you proceed through your training - Quality is more important than quantity.
Try and write about clinical encounters that mean something to you. Perhaps you found something interesting or learnt something new? Or perhaps something that was difficulty, dysfunctional, provoked some sort of emotion or reflection on your core values. - Try and structure your writing around the 13 professional competencies.
At the end of the day, it is those 13 things against which you are ultimately judged. A good way of doing this is to write about your clinical encounter or event as freely as you want first. Just get it out onto paper or the screen and do it as quickly as you can. Then step back and try and think which main professional competencies you are talking about – go through them one by one and spend about 5 seconds on each asking yourself “did this competency have a big place in this scenario I have chosen to write about”. Then restructure you written piece around the professional competencies you are demonstrating and tweak them to make them more robust (even consider using the competencies as headers to structure your write up).
- Try and write about curriculum areas where you need to provide more evidence of coverage.
For example, you may feel that you need more evidence on “Practising Ethically” or “Managing Medical Complexity” or “Community Orientation” or “Fitness to Practice” – those are the four competencies that trainees usually struggle with. - Use a short title to describe your log entry in a nutshell.
Using short titles to your log entries means you can search for a specific one much easier. For example: “Under 16y old wanting the pill with mother present” - Add your log entries in a timely way.
Don’t save them up and add them all in one go a few times a year! This looks bad because it will appear you’ve only logged stuff in time for the ARCP panels as opposed to maintaining a continuous log and continuously reflecting.
“It is not sufficient simply to have an experience in order to learn. Without reflecting upon this experience it may quickly be forgotten, or its learning potential lost. It is from the feelings and thoughts emerging from this reflection that generalisations or concepts can be generated. And it is generalisations that allow new situations to be tackled effectively.”
Gibbs (1988) Tweet
Ask your trainer to validate your ePortfolio regularly and discuss any concerns. Your trainer will not mind you reminding them.
Ask them when you have collected say 10 entries at a time. In that way – you log entries get read on time. Also, the trainer can give you feedback in an incremental way – to improve on with the next batch of log entries.
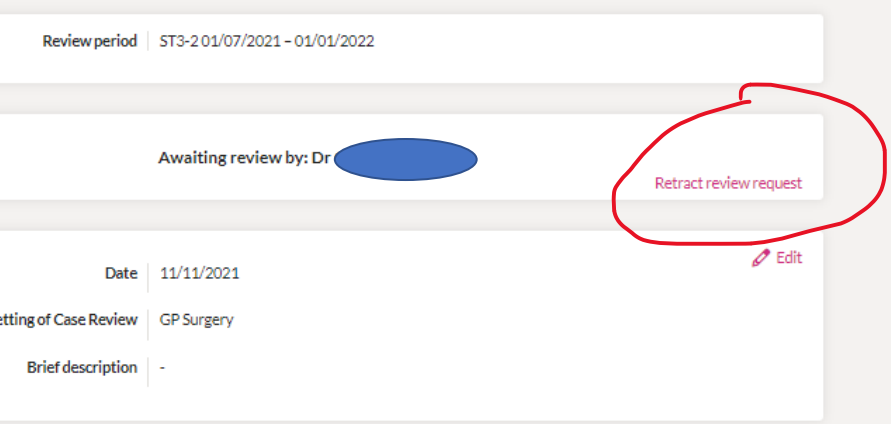
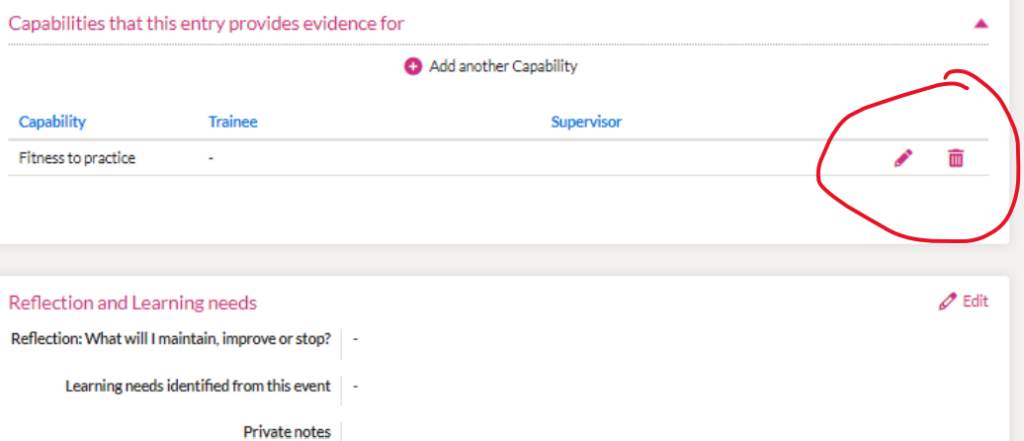
Can I edit a Log Entry once I have submitted it for review to my Trainer or CS?
Yes you can. On the right is a screenshot ( from the GP trainee perspective) that shows how the GPR can change a LLE as long as the Trainer (or the CS) does not mark it as reviewed. The Trainer can add comments & mark capabilities – but DO NOT mark it as reviewed if you want the trainee to amend it further. So, once a Trainee sends a Learning Log to a Supervisor, that entry is then locked to further editing. If it requires further changes, the TRAINEE has to retract the review request, make the changes, and then submit it for review again.
Why might the Learning Log Entry need modifying?
- Because the trainee realises there is more to add or amend.
- Because the trainer and trainee have had a discussion and from that, there is more evidence to add. Perhaps another capability or perhaps a modification of what has been written thus far.
- Because the trainer has educated the trainee on how to re-write the entry and now they want the trainee to see if they can do it.
Be warned, once the trainer or CS marks the entry as REVIEWED – then it can no longer be changed (unless through a complicated route via contacting 14 Fish).
Other FAQs
You should aim to do around…
- 3 entries per week (as a minimum) if you are in a GP post
- 2 entries per week if in a hospital post.
- The simple answer is…. as many as is appropriate. As a minimum, try and write about things that provide evidence of good performance in 3 entries.
- But the more you can do, the more evidence in your ePortfolio, and hence the better!
- BUT DO NOT MAKE SOMETHING OUT OF NOTHING. For example, don’t think that writing a one-liner about referring someone to the local support group for dementia will score you strong points for COMMUNITY ORIENTATION.
- Only write about those Professional Competences that had true meaning, depth and relevance in the particular case you are writing about.
It depends on the quality. If you have a habit of waffling on and on – then NO, it is not a good thing. You need to learn the art of conciseness, and there’s no better place than to start doing that now. Besides, it will be good for your consultation write-ups too – no doubt you might be a bit wordy in your medical notes too!
However, some of you will write long log entries because the situation was complex and had many facets you wanted to talk about. These type of long log entries tend to be more deep and meaningful and are probably log entries that might cover a number of competencies.
Just remember – quality is more important than quantity. And remember the poor person reading you ePortfolio. So, whilst it is okay to write longer entries, this is no permission to waffle on and on. Be concise and focus.
The reader does not need to know all the exact details but the relevant ones that put the experience in context. So, if your focus of the entry is something ethical or about practising holisitcally, perhaps the clinical minutiae is not so important. Can you summarise rather than spelling each bit out e.g. “Respiratory examination – a few wheezes but everything else was normal”.
However, if your focus is more clinically orientated – like Data Gathering or Clinical Management – then that’s when the specifics become more relevant. For example, if I wanted to demonstrate evidence for CEPS, I might right “Respiratory examination – left sided creps and wheezes, good air entry otherwise, no overt signs of respiratory distress, no cyanosis, RR = 20, Sats 97%, HR 78, BP 125/86, Apyrexial 36.8”
The RCGP realises that doctors have not been routinely taught to reflect. Hence, a lot of trainees struggle and often waffle on and on without truly reflecting. They end up writing long pieces that simply describe what happen without analysing it in more detail. As a result, the lengthy write up doesn’t actually demonstrate anything because it is lacking this analysis or reflection. Then, your trainer or ES can’t award you competences. And let’s not forget, the whole point of writing log entries is TO PROVIDE EVIDENCE for the competences on which you are ultimately judged.
So, as a way to help you, the RCGP have provide a structure for your learning log entry by way of boxes and headers. These boxes are meant to help you dissect a case and get you to think about it (analyse, reflect). Everyone thinks they have to write in each of the boxes – but did you know that only those boxes with an red * must be filled, the others are optional. Another thing – you do NOT have to write in a way that responds to the questions that serve as headers for each box. You can provide your own structure if you wish – I suggest you do that because what the college provides can be rather limiting when applied universally to the variety of situations we experience as doctors.
So, if you do want to use your own structure, then be sure to use your own headers. Like this…
ETHICS
He was my first patient in the morning and my consultation time had just been reduced from 30 minutes to 20 minutes. I was still quite nervous about that reduction in time and now, I had to face this chap from Romania with this language barrier. And then it got worse when I realised he was almost demanding antibiotics despite being told by the OOH service that this was not required and he needed to see a dentist. I initially felt: “Why me this morning?” I felt like running out of the consulting room. But few seconds after, I pulled myself together and asked myself: “Why not me?” The motivation that kept me through and made survive the consultations were:
- A sense of duty and respect for diversity – I had a responsibility to offer care and help to all my patient within the best of my ability irrespective of their tribe, race, religion or any other personal characteristics – i.e. without any bias.
- Empathy – This patient is clearly frustrated. I could sense he probably felt “this doctor too would not want to listen to me” or “no one wants to hear me out” or “they all don’t understand my language”. And then I began to imagine if I found myself in another country where I don’t speak their language and they don’t speak English. How would I want to be treated? This made me become patient and relaxed with him, ignore the pressure of time and the inconvenience of dealing with language problems.
- Patient safety – I did not want to rush through the consultation superficially without properly exploring the red flags. Language barriers can result in insufficient data gathering which may lead to harm. I patiently gathered my data and examine him to ensure that he is safe and is not caused harm by my action or inaction (NON-MALEFICIENCE).
As a minimum, there should be some sort of interpretation, reflection and action – and can you see that in this example? It is very clear. And this trainee clearly demonstrates some core ethical principles. By the way, this trainee was an ST1 of mine and someone graduated from Nigeria. Amazing, wouldn’t you agree? It shows you that reflection is a skill that can be taught and developed right from the start.
Oh and one last thing…. In the box future learning plans – many trainees write “I will do more reading”. Let me tell you straight up – THIS IS IRRITATING to GP educators and ARCP panel because it’s a generic comment that can be said about almost anything. You need to demonstrate that you HAVE read or done something (not that you are going to do it). So, it would better phrased “I did the BMA’s e-learning module on Language Barriers in the Consultation and I learn’t that…”. This will get you the competency of PERFORMANCE, LEARNING & TEACHING, whereas the former gets you nothing and is a waste of space! So, if you are going to read or use another educational resource, explicitly state which resource you are going to read rather than ‘A book on Dermatology’. The explicitness tells us that you’ve really thought about it.
It is important to make evident any emotional context to the learning log entry and reflect why this might be plus your past experiences of similar situations and the views of others (be this colleagues or the medical evidence base).
Remember, earlier we said that LEARNING cannot happen without REFLECTION. And part of REFLECTION involves SELF-AWARENESS and that means being aware of your thoughts and emotions. It’s only through examining how something made us feel can TRANSFORMATIVE NEW LEARNING happen. Isn’t that what you want?
So, whilst we understand trainees are a bit scared of sharing their thoughts and feelings, also understand that Trainers, Educational Supervisors and ARCP panel consider those who share their inner thoughts and feeling to be mature adult deep-thinking learners. And we love that. We do not interpret someone as weak when they share their thoughts and feelings. We do not think badly of you. Instead, what we think is something positive – that it takes a motivated trainee who truly wants to better themselves to talk about their feelings. So…. go on, have a go. See what the reaction is.
Do not save up your entries – they will have lost some of their value to you by the time you do find time to expand on them. Write them there and then – whilst everything is fresh in your mind and whilst the case excites you. Write them any later – and you wont remember it so well, you’ll hate writing it up and your initial momentum will have gone.
Also it’s unfair to land your GP Trainer or Educational Supervisor with 30+ entries all in one go shortly before your ES meeting. Think about it. How would you feel if you have many things to do in both your work and personal life, but then to be landed with a number of long’ish entries to read plus a deadline that it must all be done within 2 weeks “before my ES meeting”. Would you be happy?
So do it all in a timely way, so that your GP Trainer or ES can also read them in a more gradual, relaxed and timely way too. And besides, doing it this way means the GP Trainer or ES can give you advice and feedback on your entries and help you tweak them to make them better (and thus help you to reflect better in real life).
The process of using learning logs involves developing thinking and learning skills. This can be super-enhanced by a peer partnership system. So, how about forming a peer system with one-two-three-or four others. In this peer system, the trainees would be encouraged to discuss and share their thoughts, as well as to develop their learning logs in a collaborative way.
The advantage is that by the other mindsets within the group would expand your thinking even further. Anyway, it’s just a thought. Perhaps something worth developing at HDR – talk to your Training Programme Directors.
The bottom line is that the college says it should be the Educational Supervisor that reads your log entries.
HOWEVER…
There is an incredible amount of work the Educational Supervisor has to do when it comes to your reviews.
- So, we think it is more practical if your GP Trainer reads them if you are in a GP post. And here are our reasons why…
They see your day-to-day work anyway and it’s good for them to get a better feel about you based on what you write about the day-to-day experience. A good proportion of the ePortfolio entries will have been discussed with the trainer already. That places the trainer in an ideal position to more reliably validate log entries against the competencies. Also, the trainer can read the entries in a progressive way throughout the 6 month attachment. That means they can also provide feedback in an progressive and incremental manner rather than a whole mass of feedback being dumped on you by the Educational Supervisor. We hope this will enable you, the trainee ,to develop better reflective skills in a progressive manner too. Finally, continuously reviewing how their trainee is engaging with their ePortfolio provides the trainer with another informal form of assessment on how the trainee is progressing (through their level and depth of reflection as well as active engagement). - In a hospital post, encourage your hospital consultants to read some. Many won’t because they are busy or don’t understand how to map your learning logs to the Professional Competencies (and actually, they may not understand some of the competences – after all, they are consultants in the hospital world, not the GP world). That leaves the Educational Supervisor (ES) to read the rest.
- Once you have a set of 10 log entries – email or ask your Trainer/ES to read them. Don’t leave it all til the end when they may have 60 to read in a very short space of time. That’s unfair – please think about them.
- What I do with my trainee, which might help some of you, is to periodically (say once every 6-8w) hijack the tutorial to look at the ePortfolio entries, read them and see what we can learn from them.
- I also ask my Practice Manager not to cancel the block of tutorial time when the trainee is away on annual or sick leave. That gives me protected time again to look at and review their ePortfolio.
- And many Deaneries have now made it the rule that every GP trainer must be provided 1 hour PROTECTED GP training admin time a week. This hour SHOULD NOT be squeezed in by your Practice Manager. Instead, it should be in placement of surgery time. And this time provides an ideal opportunity to read some entries and other GP training stuff.
Trainees who are poor or extremely reluctant to write are often mistakenly characterised as either lazy or poor thinkers. But this could not be further from the truth. You may find that these reluctant writers,
- aren’t willing to note ideas in a Learning Log because they are sharing personal perceptions, feelings and thoughts.
- aren’t willing to include emotional stuff for fear of being judged.
- aren’t willing to show their learning gaps for fear of being judged as incompetent.
- simply lack writing skills in English – especially if they are not native to the UK.
- have too much other stuff going on in their lives that failing to engage with Learning Logs is one of many indicators that suggests they are struggling. eg going through a divorce, being in debt and working every hours God sends, being sued, alcohol, drugs, relationship problems, child custody problems and so on.
- Medical problems like anxiety, depression, bipolar, chronic pain, and so on.
SO – DON’T JUDGE THE FAILURE TO ENGAGE. THE FAILURE TO ENGAGE SHOULD MAKE YOU WANT TO OPEN UP A DIALOGUE ABOUT WHAT IS HAPPENING FOR THE TRAINEE (SO THAT YOU MIGHT BE ABLE TO HELP THEM BETTER). RDMp them – if you’re unfamiliar with this term, look up RDMp on the BRADFORD VTS pages on ‘THE TRAINEE IN DIFFICULTY’.
One final things - please anonymise!
Anonymise all staff & patient identifiable information. If you do not then you are not only breaching confidentiality but you can land yourself in trouble.
