

Women's Health
Bradford VTS Clinical Resources
- by Dr Ramesh Mehay
- Last modified: 29th April 2024
- No Comments
Home » CLINICAL KNOWLEDGE » womens health
DOWNLOADS
path: WOMEN’S HEALTH
- adolescent gynaecology.pptx
- amenorrhoea.doc
- ammenorhoea and intermenstrucal bleeding IMB.doc
- antenatal care.pdf
- antenatal monitoring timelines.doc
- antenatal monitoring.pdf
- antenatal screeing timeline.pdf
- antenatal screening tests.pdf
- breast cancer.doc
- breast feeding.doc
- breast problems.doc
- cervical cancer and hpv.ppt
- cervical screening and wilsons criteria.ppt
- cervical smear – everything you wanted to know.pdf
- cervical smear – how to take a sample.pdf
- cervical smear – managing the result.pdf
- cervical smear results explained.pdf
- cervical top tips 2019.pdf
- chlamydia handout.doc
- contraception – a comprehensive guide with cases.ppt
- contraception – a comprehensive summary.pdf
- contraception – accidental pregnancy in first year of use.ppt
- contraception – advising women on contraceptive options.pdf
- contraception – choices.pdf
- contraception – coc tutorial
- contraception – emergency – post coital counselling.doc
- contraception – emergency – post coital IUCD counselling.doc
- contraception – emergency assessment.pdf
- contraception – implanon training theory.pdf
- contraception – indications for emergency contraception.ppt
- contraception – LARC in a nutshell from NICE bites.pdf
- contraception – the pill in practice.ppt
- contraception – ukmec full 2016.pdf
- contraception – ukmec summary 2016.pdf
- contraception – what to prescribe.doc
- contraception – what to prescribe.docx
- contraception and family planning.ppt
- contraception case.doc
- contraception for gp trainees.pptx
- contraception in general practice – cornwall.doc
- contraception oral – what to give when.rtf
- contraception quiz with answers.doc
- contraception tutorial plan and cases.doc
- contraceptive pills.ppt
- ctg – cardiotocography.pdf
- curriculum for o&g.doc
- cystitis.ppt
- edinburgh postnatal depression scale.pdf
- gynae problems in general practice – tutorial plan.doc
- gynae quick tips.doc
- hrt – tailoring it to the patient.ppt
- hrt – the best guide to prescribing esp last two pages.pdf
- hrt – which one to give.doc
- hrt and patient compliance.pdf
- hrt and perimenopausal women.pdf
- hrt and postmenopausal women.pdf
- hrt in general practice – tutorial plan.doc
- HRT made easy 2023.pdf
- hrt prescribing.doc
- hrt protocol – moorside surgery.doc
- infertility – an overview for gp.ppt
- infertility management.pptx
- infertility test values.pdf
- menopause assessment and giving hrt.doc
- menopause symptoms.pdf
- menorrhagia – managing.ppt
- menorrhagia.pdf
- menstrual problems and cases.doc
- obstetric abdominal palpation.ppt
- obstetric case – cholestasis.doc
- obstetric examination.pdf
- obstetrics – chicken pox in pregnancy.doc
- postcoital bleeding – management.doc
- postnatal 6w check – what you should do.pdf
- postnatal depression scale – edinburgh.pdf
- pregnancy symptoms.pdf
- screening in pregnancy.pdf
- thrush – vaginal candida.doc
- top tips in womens health.pdf
- vaginal discharge – table of differentials.pdf
- vaginal discharge.doc
- vaginal examination – some rules and advice.ppt
- vaginal gynae examination checklist.doc
- vulval carcinoma.ppt
- womens health in family medicine.pdf
- womens health osce stations.doc
WEBLINKS
- Primary Care Women’s Health Forum – full of excellent top tips, videos, webinars and other resources
- Gynae & Breast super-condensed curriculum – what you should know (RCGP)
- OSCEs in Obs & Gynae (BVTS)
- Perinatal Mental Health Toolkit (RCGP)
- NHS Cervical Screening Programme www.bsccp.org.uk,
- ELFH module – NHS cervical screening programme e-lfh.org
- BAD patient-information-leaflets
- British Society Study of Vulval Disease
……………………………………..
Information provided on this medical website is intended for educational purposes only and may contain errors or inaccuracies. We do not assume responsibility for any actions taken based on the information presented here. Users are strongly advised to consult reliable medical sources and healthcare professionals for accurate and personalised guidance – especially with protocols, guidelines and doses.
COME AND WORK WITH ME… If you’d like to contribute or enhance this resource, simply send an email to rameshmehay@googlemail.co.uk. We welcome collaboration to improve GP training on the UK’s leading website, Bradford VTS. If you’re interested in a more active role with www.bradfordvts.co.uk (and get your name published), please feel free to reach out. We love hearing from people who want to give.
……………………………………..
Some basics
- Heavy bleeding – estimate how much bleeding – what size clots (2p?), how many pads/tampons per day.
- Always ask about Intermentstrual Bleeding (IMB). If present – it warrants further Ix.
- Dyspareunia (painful sex) is another important thing to ask about.
- Don’t dismiss Teenagers – take them seriously. Take a good history. They may have endometriosis or adenomyosis. Both repsond well to hormone thereapy. If missed >>> fertility problems later on in life.
- Vulval itch – try and examine these ladies and don’t just think candida. Exclude Lichen Sclerosis, VIN and VSCC.
- Abdo pain – ALWAYS exclude ectopic pregnancy in a female of fertile age with abdo pain.
- Abdo pain in pregnancy – most cases will be harmless. But do make sure you exclude abuption, preterm labour and appendicitis.
- PCOS – lots of ladies have it and don’t forget this puts them at risk of endometrial cancer and metabolic dsorders like diabetes and dyslipidaemia. HbA1C, Lipid Profile, BP yearly.
- Ovarian Cancer – think in persistent or worsening intra-abdominal symptoms – like pain, IBS type symptoms, abdo swelling/bloating. Ca125 does not rule out ovarian Ca. Always think of in the middle aged lady with a large abdo.
- Persistent IMB over age 40 – think endometrial cancer. But also think of it in younger ages if they have risk factors (e.g. PCOS).
Pregnancy at a Glance
- Patient’s seem unaware that in general, 1 in 4 pregnancies will end in a miscarriage
- In women <30y, 1 in 10 pregnancies end in miscarriage (10%)
- In women 35-39y, 2 in 10 pregnancies end in miscarrage (20%)
- In women 40-44y, 3 in 10 pregnancies end in miscarriage (30%)
- In women over 45y, 5 in 10 pregnancies end in miscarriage (50%)
Success of IVF (Live Birth Rate)
- Under age 35: 45%
- Ages 35-37: 33%
- Ages 38-40: 20%
- Ages 41-42: 10%
- Age 45: 3%
Please note that Live Birth Rate is not the same as Positive Pregnancy Test Rate (latter is higher, obviously).
- Discuss smoking cessation, alcohol intake, weight management, exercise
- Discuss nutritional advice – care with dairy produced, tinned meats etc
- Prescribe folic acid intake: usual dose for most women trying to get pregnant and during the first 12 weeks of pregnancy is 400 micrograms, taken once a day.
- Remember higher dose Folic acid 5mg od if
- BMI >30,
- if diabetic,
- family history or past history of NTD,
- if taking anti-epileptic medication
- in multiple pregnancies.
- Medication review
- Mental health and emotional wellbeing review
- Aspirin taken from the first trimester can improve placental blood flow and therefore fetal growth.
- It reduces stillbirth risk, prevents pre-eclampsia and associated preterm delivery.
- Midwives will use the risk assessment tool when deciding if aspirin is required, please continue prescriptions when requested.
- More placentas are now being sent for histology. If there is evidence of placental dysfunction or insufficiency, then aspirin will be recommended for future pregnancies. Look for recommendations in the snowdrop (pregnancy loss) clinic letters.
- See the Bradford Royal Infirmary risk assessment for deciding who to give aspirin to throughout pregnancy:
- Have a look at The Leicester Guidance (2019) – in particular, appendix 1 based on NICE guidelines (2019) and Saving Babies Lives (2019)
- ALWAYS ask women before and after birth about their mental wellbeing and consider their mental health history. Past history is important in identifying women at high risk of mental illness and should be considered for referral.
- Fluoxetine is the safest SSRI in pregnancy.
- Sertraline is the safest during breastfeeding a full term, healthy baby.
- Psychotropic medication should not be stopped because of pregnancy but it is important to consider risks/benefits and seek advice.
Menopause & HRT at a Glance
A lot of people think menopause is when you have hot flushes and night sweats. But actually there are other more common symptoms and you might have these rather than the night sweats and flushes. So have a look at the list below and if you have some of these chat with your GP about the menopause and the possibility of body-identical HRT.
So, of course many women will get hot flushes and night sweats, but many don’t and they get a combination of the symptoms on the right…
A useful self-check for patients is the Newson Menopause Symptom Questionnaire
Symptoms other than Hot flushes & Night Sweats
- Tiredness and fatigue (exhausted)
- Brain Fog – an inability to focus. Lapses in memory.
- Feeling ‘flat’ and down. Mood swings. 7 in 10 women get ‘meno-rage’ with irritability and guilty feelings. Trouble concentrating and trouble with sleep. Lack of motivation.
- Bloating/Water retention
- Swollen tummies and puffiness
- Sore/tender breasts
- Vaginal dryness – the 4th most common menopause symptom
- Dry eyes, dry mouth, sore lips.
- Low sex drive. May mean u need testosterone as well. Ask your GP.
- Headaches & Dizziness
- Muscle body aches all over the body. Joint pains.
- Feeling cold – “cold flashes”
- Weight gain – It can be hard to lose weight in your 40s and 50s due to the change in hormone balance. If you’re on a diet programme, like slimming world, perhaps hrt will help your losses.
- Bladder Weakness and recurrent urine infections.
- Thinning hair – A decline in progesterone and estrogen causes hair follicles to loosen.
- Acne – in 15% of women aged 50 +.
- Changes in skin texture – loss of 30% of its collagen during the first five years of menopause. After that, the decline is more gradual with 2% sloping off every year for the next 20 years. Leads to itchy skin and sagging breasts.
- An odd body odour.
- Brittle nails.
- Tingling in the arms/legs – small electric shocks on your skin, as though you have had a static charge from rubbing a balloon on your head. Burning mouth.
- Tinnitus
- Shortness of Breath
Major risk factors are
- BMI ≥ 40 and
- hereditary conditions such as Lynch or Cowden syndrome.
Minor risk factors include
- BMI 30-39,
- diabetes and
- polycystic ovarian syndrome (PCOS).
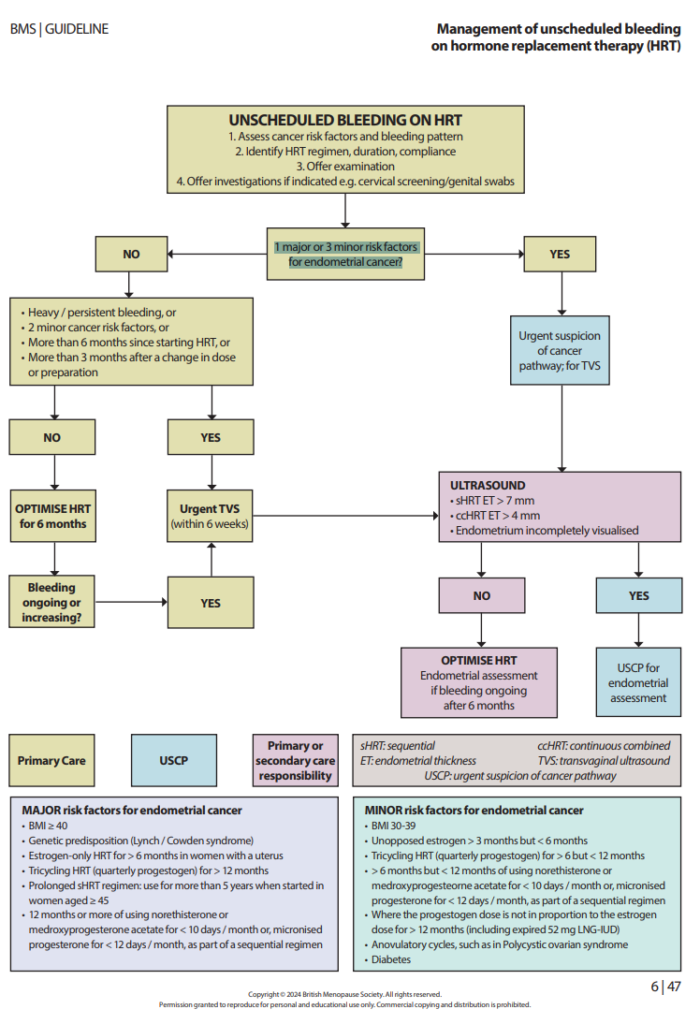
Optimisation of modifiable factors can, in themselves, reduce episodes of unscheduled bleeding on HRT and endometrial cancer risk.
Risk factors for endometrial hyperplasia and cancer, independent of HRT, should be identified.
If a patient on HRT has unscheduled bleeding
Refer urgent if
- 1 major risk for endometrial cancer or (i.e. BMI ≥ 40 and/or has Lynch or Cowden Syndrome)
- 3 minor risk factors for endometrial cancer (i.e. BMI 30-39 + Diabetes + PCOS)
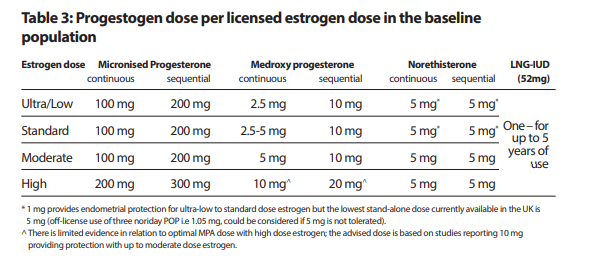
Unbalanced estrogen to progestogen dose
British Menopause Society (BMS) guidance(25) recommends a progestogen dose in proportion to the estrogen dose in people who have a uterus, to reduce unscheduled bleeding and endometrial cancer risk. The table on the right summarises this section
and outlines the progestogen dose that appears to provide adequate endometrial protection for different strengths of licensed estrogen dosages (ultra-low, low, standard, moderate and high).
- x
- x
x
x
x
Cervical Things at a Glance
HPV Gardasil vaccination
- Offered to girls and boys in year 8 (age 12/13) – 2 doses.
- Very safe and very effective. If parents anxious that it may promote early sexual activity, please reassure them that this is not the case and that this is a cancer preventing vaccine.
- Not just cervical but vulval, anal, penile and some oropharyngeal cancers. Also offers protection against genital warts.
- Do encourage young people with LD to take up screening as there is low uptake
HPV infection
- HPV 16 and 18 cause about 70% of all cervical cancers. HPV screening looks for these and another 12 ‘high risk’ subtypes.
- Patients are often anxious about an HPV positive result and are concerned about partner fidelity. Patients should be reassured that it is a very common infection that can be transmitted by digital as well as genital contact and does not imply infidelity.
- They may have been first exposed months or years previously. There is no treatment but patients with a normal immune system will clear the virus in time (90% within 2 years).
- A ‘cervical smear’ is taken in the same way as previously. HPV testing is now the primary screen.
- If HPV negative, the patient continues with routine screening at 3 or 5 years depending on age.
- If HPV positive, cytology is performed. Patients with any grade of dyskaryosis are referred to colposcopy.
- Patients whose screen is HPV positive but cytology negative will be invited to have a repeat screen in 12 months.
- PCB is rarely caused by cervical cancer and on its own does not always warrant a fast track referral
- Contact bleeding on taking swabs or a smear does not suggest serious disease is more likely
- Consider infection (especially chlamydia in young women) as a possible cause
- In the presence of a normal screening history and a normal looking cervix, cervical cancer can effectively be excluded
- Consider Fast Track referral in women with PCB when the appearance of the cervix is suggestive of cervical cancer or in women with persistent and unexplained PCBx
- IMB in the absence of PCB is very unlikely to be caused by cervical disease and is more likely to be due to an endometrial problem (especially in older women or women with associated heavy or irregular periods) or a contraceptive problem (especially the implant or POP)
- Investigation with a pelvic ultrasound or outpatient hysteroscopy may be more appropriate than colposcopy but in young women with a normal examination, hormonal manipulation is reasonable before investigation
Polyps and Cysts
- Nabothian cysts are normal – multiple ones can look odd but they do not need treatment or referral to colposcopy
- Small benign looking polyps can be referred routinely. A post LLETZ cervix can sometimes look odd with a rather prominent polypoid ‘ectropion’ – please familiarise yourself with this appearance
Ectropion
- Asymptomatic ectropions do not need treating – they are a normal feature
- Patients with normal looking ectropions that are causing a bothersome discharge (with negative swabs for infection) or post-coital bleeding can be referred routinely to colposcopy
- Please ensure the patient is not overdue cervical screening as we cannot treat the ectropion without it.
Referrals for Colposcopy
- Please ensure date and result of last smear is included in any referral letter to colposcopy.
- If a smear is due, please take one but do not delay an urgent referral to wait for the result.
- www.bsccp.org.uk (for guidanceguidance, webcasts and images)
Vulval Things at a Glance
The History
A good history can indicate a potential diagnosis such as eczema, psoriasis, candida, lichen sclerosus, lichen Planus
- Itch, soreness (feeling cut), dysuria, PV Discharge, perianal soreness/itch
- How long has patient had symptoms?
- What do they wash with?
- Any history of skin problems?
- Any autoimmune conditions?
Take your time and listen carefully
Use interpreting services if non-English speaking (not a family member)
Always examine children who have symptoms of itch or soreness (exclude abuse)
The Examination
When examining the vulva check signs of:
- Any architectural change of vulva
- Silvering/whiteness
- Erythema
- PV Discharge (take a swab if suspected candida)
- Erosions
- If you see a lesion with symptoms of itch and soreness or a crusty-type lump
- Don’t always assume vaginal candida – confirm diagnosis by vaginal swab or vaginal or vulva examination
- Recurrent Vaginal Candida: 4 episodes in 12 months – 2 confirmed by culture
- Vaginal candidiasis is unlikely in post-menopausal women
- Vulva problems are not age-related, conditions such as lichen sclerosus can affect younger girls
- Demarked area of erythema on mons pubis could be psoriasis
- Loss of architecture and silvering/paleness of the vulva could indicate lichen sclerosus
- Advise women to avoid feminine hygiene products, avoid washing with shower gels/soaps
- Advise use of an emollient such as Cetraben / Diprobase / Aveeno as a soap substitute applying before or after showering. This can be applied to toilet paper each time the woman goes to the toilet and more frequently if needed.
- Prescribe a potent steroid such as clobetasol ointment.
- Apply one fingertip each morning for 2 weeks.
- Then apply one fingertip steroid alternative mornings for a further 2 weeks.
- Continue with one fingertip of steroid to be applied 1-2 times a week.
- Review patient, if no improvement refer to Vulva Clinic.
- Wear white 100% cotton underwear
- Avoid tight clothing such as tights
- Double-rinse clothing
- Wash with warm water and soap substitutes
- Avoid all fragranced soaps or sprays
- Avoid bubble baths and washing hair in the bath
- Refer if unsure of diagnosis or would like expert advice to Community Vulva Service at Shipley (if you are based in Bradford)
- If you want to do a Fast Track Referral: please refer under 2ww FastTrack EVEN if under the care of Vulva Service.
- Try to avoid steroid if unsure of diagnosis prior to referral and use moisturiser only
Ramadan & Fasting Advice for Pregnancy
Fasting is an obligation for competent, healthy adult Muslims although there are exemptions. Many of those who could seek exemption might still want to fast. It is important to respect this but it is advisable to start planning 6-8 weeks before Ramadan to avoid adverse outcomes e.g. patient self-adjustment of medication.
Who is exempt from fasting?
- Acute or chronic illness
- Travellers
- Pregnant/breastfeeding*
- Menstruating/postpartum bleeding
- Children
- Mentally unwell/lacks capacity
*Consensus by Islamic scholars that it is permissible not to fast if there is threat of harm to mother/child
The fast of Ramadan lasts from dawn to sunset for a period of 29 or 30 days. It follows the lunar calendar so is brought forward by about 10 days each year. Fasting people generally eat two meals a day: often a smaller meal before dawn (Suhoor) and a larger one after sunset (Iftar). No fluids or food are taken during daylight hours. This includes water and most medication.
Permissible interventions/medications
- Blood tests
- Vaccinations
- Asthma inhalers*
- Ear drops*
- Eye drops
- Transdermal patches
*Difference of opinions exist. Encourage patients to contact their local imam, or BIMA for advice.
Should I advise my patient not to fast?
BIMA have an interactive traffic light tool that help to classify patients into low/moderate risk, high risk, and very high risk at
- www.britishima.org/Ramadan-compendium
- in chapter 6.
Patients in the two higher tiers should be advised that they ‘must not fast’ and ‘should not fast’ respectively. Consider advising these patients to fast in the shorter winter months. If they insist to fast, monitor regularly and ask that they should be prepared to break the fast in case of adverse events. Below is a shortened summary of the advice:
MUST NOT FAST
V. HIGH RISK
- Severe underlying medical condition
SHOULD NOT FAST
HIGH RISK
Any patient in first trimester
INDIVIDUAL DECISION - WHAT IS THEIR ABILITY TO TOLERATE IT - LOW RISK
- Uncomplicated healthy in second/third trimester

